
![]()
Unrecognised oesophageal intubation
OVERVIEW
Esophageal intubation occurs when an endotracheal tube (ETT) is mistakenly inserted into the esophagus instead of the trachea. If this error is not immediately detected, it is termed unrecognised oesophageal intubation.
Unrecognised oesophageal intubation leads to failure of alveolar oxygenation and ventilation, and gastric insufflation. The effects can be catastrophic:
- severe hypoxia and hypercapnea, and cardiac arrest (~15x risk)
- gastric distention, regurgitation, and aspiration (~15x risk)
Much of this CCC entry is derived from the PUMA guidelines on unrecognised oesophageal intubation by Chrimes et al (2022).
FREQUENCY
Worldwide, 5.6% of critically ill patients undergoing intubation attempts had an esophageal intubation in the INTUBE study (Russoto et al, 2021)
- Capnography was NOT used in 69% of these cases
The NEAR study (Brown et al, 2014) found that inadvertent esophageal intubation occurred in 3.4% of attempted intubations performed in US, Canadian and Australian EDs.
- 4% of esophageal intubations were unrecognized
The NAP4 study in the UK found that capnography was not used in >75% of unrecognized esophageal intubations and contributed to 77% avoidable deaths related to tracheal intubation among critically ill patients (Cook et al, 2014)
- Unrecognised oesophageal intubation is much more likely to occur in the ED and the ICU than in operating theatres (by up to 100-fold).
CAUSES OF OESOPHAGEAL INTUBATION
Misidentification of larynx (Chrimes et al, 2022)
- Limited operator expertise/Inadequate supervision
- Practitioner complacency
- Compromised performance
- Compromised laryngeal view
- Distorted glottic anatomy
- Glottic impersonation (see Figure 1)
- Equipment issues
Delivery issue (Chrimes et al, 2022)
- Tube, introducer or bronchoscope not passed into trachea or displaced during railroading
- Blind intubation via supraglottic airway
Movement after successful tracheal placement (Chrimes et al, 2022)
- Withdrawal of bougie, stylet or flexible bronchoscope
- Subsequent airway instrumentation
- Patient coughing or moving
- Chest compressions
- Changes in patient position
- Paediatric patients
- Poorly secured tube
Failure to recognise oesophageal intubation (Chrimes et al, 2022)
- CO2 detection not available/used/functioning
- Failure to confirm CO2 detection
- Spurious CO2 detection
- False-positive CO2 detection using colorimetry
- CO2 detection in association with oesophageal intubation
- Misinterpretation of monitoring display:
- Confusion of airway pressure waveform with capnography waveform
- Failure to acknowledge the potential for absence of sustained exhaled CO2 to indicate oesophageal intubation.
- Cognitive biases
- Knowledge deficits
- Communication deficits

PREVENTION
Oesophageal intubation can be prevented during laryngoscopy by (Chrimes et al, 2022):
- Routine use of a videolaryngoscope (improves glottic view; allows other team members to confirm what is seen)
- Deliberate, sequential exposure of anatomy during laryngoscope blade insertion to avoid ‘overshooting’ the larynx (e.g. identify the epiglottis – “the gateway to the larynx” – before advancing to the vallecula to expose the glottic opening)
- State the view during any laryngoscopy attempt (e.g. “I can see the epiglottis, the back of the vocal cords and the arytenoids:“)
RECOGNITION OF OESOPHAGEAL INTUBATION
Oesophageal intubation can be recognised by the following measures (Chrimes et al, 2022):
- Use of waveform capnography and pulse oximetry for all episodes of airway management.
- Carefully observe and verbally confirm ETT placement (e.g. state “ETT between the vocal cords and anterior to the arytenoids”) before laryngoscope removal
- Identify breath-by-breath CO2 exhalation on waveform capnography, thus confirming alveolar ventilation.
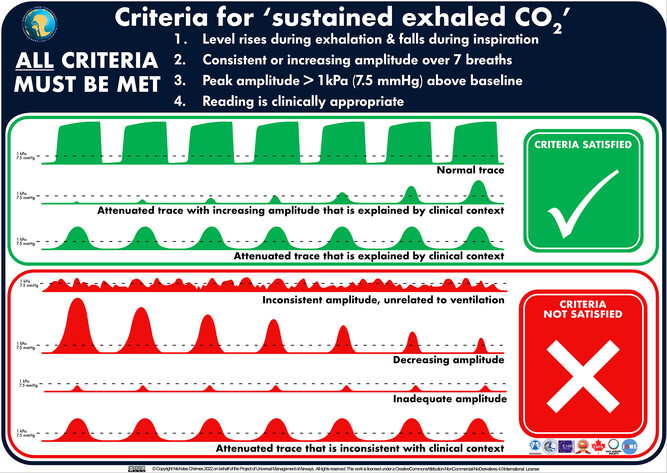
- Ensure these criteria are met for confirmation of “sustained exhaled CO2” (see Figure 2):
- Amplitude rises during exhalation and falls during inspiration.
- Consistent or increasing amplitude over at least 7 breaths.
- Peak amplitude more than 1 kPa (7.5 mmHg) above baseline.
- Reading is clinically appropriate.
- The airway operator and assistant should each independently check and then verbalise that, for example, “”sustained exhaled carbon dioxide” and adequate oxygen saturation are present/ absent”.
Tips and pitfalls
- If oesophageal intubation is recognised early (e.g. absent or inadequate ETCO2 waveform) it is NOT necessary to deliver 7 breaths before removing the ETT – at least 7 breaths are only required to exclude oesophageal placement.
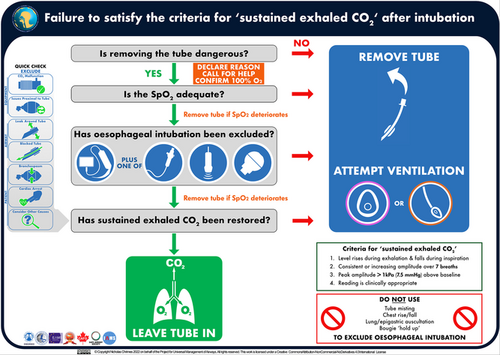
ACTIONS REQUIRED WHEN “SUSTAINED EXHALED CO2” CANNOT BE CONFIRMED
Inability to detect “sustained exhaled CO2” requires oesophageal intubation to be actively excluded (Chrimes et al, 2022).
- The default response should be to remove the tube and attempt ventilation using a facemask or supraglottic airway.
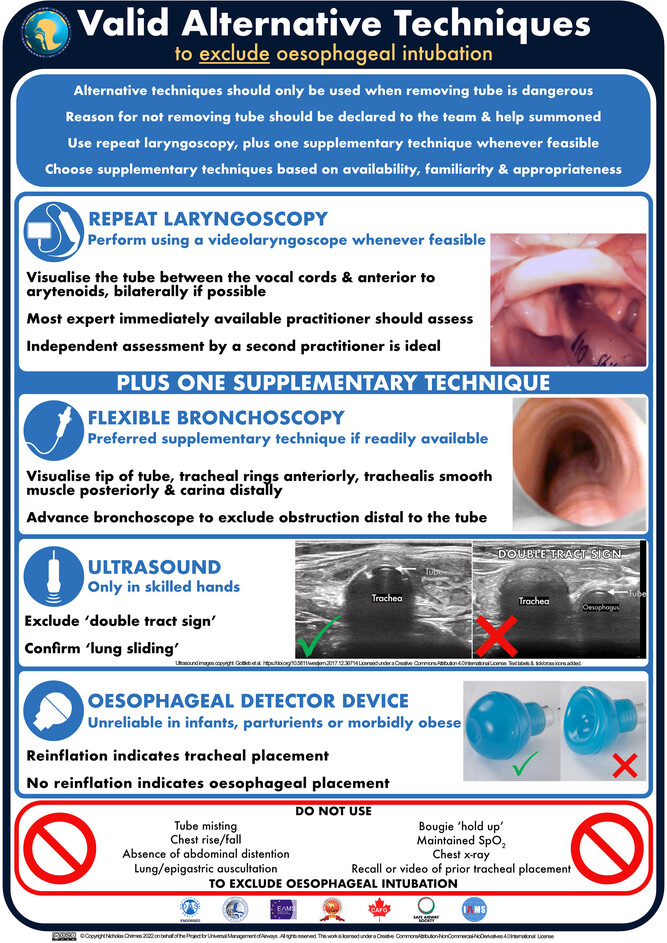
- If immediate tube removal is not undertaken (because removing the ETT is considered dangerous and SpO2 is maintained), call for help and actively exclude oesophageal intubation using valid techniques (see Figures 3 and 4):
- repeat laryngoscopy (use VL, ideally confirmed by a second expert intubator)
- flexible bronchoscopy (identify ETT tip, tracheal rings, trachealis, and carina and exclude distal obstruction)
- Ultrasound, if skilled, to identify lung sliding and exclude the “double tract sign”
- use of an oesophageal detector device (~1/20 false positive rate; unreliable in infants, late pregnancy, and severe obesity)
- Do NOT use clinical examination to exclude oesophageal intubation.
Tube removal should be undertaken if any of the following are true (Chrimes et al, 2022):
- Oesophageal placement cannot be excluded
- Sustained exhaled carbon dioxide cannot be restored
- Oxygen saturation deteriorates at any point before restoring sustained exhaled carbon dioxide
Tips and pitfalls:
- In the absence of sustained exhaled CO2, it is almost always more dangerous to NOT remove the ETT than it is to remove it
- Never assume that cardiac arrest or severe bronchospasm are reasons for lack of exhaled CO2 detection – they are recurrent themes in fatal cases of unrecognized esophageal intubation (Chrimes et al, 2022)
- During CPR for cardiac arrest, ETCO2 <7.5 mmHg (1 kPa) either indicates an incorrectly placed ETT or a very high likelihood of a poor outcome from resuscitation regardless.
- In bronchospasm (e.g. severe asthma, anaphylaxis) ensure ventilation with adequate inspiratory pressure (e.g. override pressure release valve on bag-valve apparatus) and expiratory time when checking for “sustained exhaled CO2”.
CLINICAL TESTS FOR DETECTION OF OESOPHAGEAL INTUBATION
Clinical examination should not be used to exclude oesophageal intubation (Chrimes et al, 2022). This is because clinical tests are all significantly inferior to waveform capnography for recognition of oesophageal intubation (Hansel et al, 2023)
- Colorimetric capnography is the next best alternative to waveform capnography
- If no capnography is available, consider using an oesophageal detector device (though it still has a 1 in 20 miss rate)
- Hansel et al (2023) performed a systematic review of 49 studies involving 10,654 participants to determine the false positive rate of clinical tests (see table), with waveform capnography (or bronchoscopy) considered the gold standard.
However, clinical examination may help recognise esophageal intubation if findings consistent with tracheal placement are absent.
| Test and false positive rate (FPR) (95%CI) | Finding suggesting tracheal placement |
| Misting FPR = 0.69 (0.43–0.87) | presence of misting or condensation inside the tube or catheter mount during exhalation |
| Lung auscultation FPR = 0.14 (0.08–0.23) | presence of breath sounds auscultated with a stethoscope, usually bilaterally at the axillae |
| 5-point auscultation FPR = 0.18 (0.08–0.36) | Lung base and apex auscultation, combined with epigastric auscultation with the presence of breath sounds in all areas except the epigastrium |
| Chest rise* | Observation of the chest wall during attempted lung ventilation with chest rise |
| ‘Hang-up’* | Advancement of a long narrow airway device to at least 30 cm depth results in resistance detected |
| Oesophageal detector device FPR = 0.05 (0.02–0.09) | A low-cost device that attaches to the end of the tube, consisting of either a compressible bulb (self-inflating balloon) or a 50–60 ml syringe.The balloon refills within a few seconds or air is readily aspirated into the syringe. |
* insufficient evidence to determine true FPR
POTENTIAL CONFOUNDERS
Reasons for CO2 detection following oesophageal intubation (Chrimes et al, 2022):
- No alveolar ventilation occurring
- Prior ingestion of carbonated beverages or antacids
- Gastric insufflation of CO2 for upper gastrointestinal endoscopy
- Prolonged ventilation with facemask or poorly positioned supraglottic airway before attempting tracheal intubation
- Bystander rescue breaths
- Some alveolar ventilation potentially occurring
- Tracheo-oesophageal fistula with tube tip proximal to fistula
- Proximal oesophageal intubation with uncuffed tube in a paediatric patient
Note that none of these potential confounders meet all 4 criteria (described above) for a “sustained ETCO2 waveform”.
Reasons why SpO2 may be preserved following oesophageal intubation (Chrimes et al, 2022):
- Oesophageal intubation following the use of techniques to extend the safe apnoea time
- Oesophageal intubation in the presence of spontaneous ventilatory efforts. These patients precipitously deteriorate following subsequent administration of neuromuscular blocking agents.
- Proximal oesophageal intubation with leak around uncuffed tube or tube with deflated cuff (particularly with small diameter tracheal tubes in paediatric patients)
- Tracheo-oesophageal fistula with tip of tube proximal to fistula
As with clinical examination, pulse oximetry cannot be used to exclude oesophageal intubation, but early recognition of desaturation may aid in its diagnosis (Chrimes et al, 2022).
CONCLUSION
These are the key recommendations from the PUMA guidelines by Chrimes et al (2022):
- Exhaled carbon dioxide monitoring and pulse oximetry should be available and used for all episodes of airway management.
- Routine use of a videolaryngoscope is recommended whenever feasible.
- At each attempt at laryngoscopy, the airway operator is encouraged to verbalise the view obtained.
- The airway operator and assistant should each verbalise whether ‘sustained exhaled carbon dioxide’ and adequate oxygen saturation are present.
- Inability to detect sustained exhaled carbon dioxide requires oesophageal intubation to be actively excluded.
- The default response to the failure to satisfy the criteria for sustained exhaled carbon dioxide should be to remove the tube and attempt ventilation using a facemask or supraglottic airway.
- If immediate tube removal is not undertaken, actively exclude oesophageal intubation: repeat laryngoscopy, flexible bronchoscopy, ultrasound and use of an oesophageal detector device are valid techniques.
- Clinical examination should not be used to exclude oesophageal intubation.
- Tube removal should be undertaken if any of the following are true:
- Oesophageal placement cannot be excluded
- Sustained exhaled carbon dioxide cannot be restored
- Oxygen saturation deteriorates at any point before restoring sustained exhaled carbon dioxide
- Actions should be taken to standardise and improve the distinctiveness of variables on monitor displays.
- Interprofessional education programmes addressing the technical and team aspects of task performance should be undertaken to implement these guidelines.
REFERENCES
LITFL.com
- CCC – Direct laryngoscopy
- CCC – Video laryngoscopy
Journal articles
- Brown CA 3rd, Bair AE, Pallin DJ, Walls RM; NEAR III Investigators. Techniques, success, and adverse events of emergency department adult intubations. Ann Emerg Med. 2015 Apr;65(4):363-370.e1. doi: 10.1016/j.annemergmed.2014.10.036. Epub 2014 Dec 20. Erratum in: Ann Emerg Med. 2017 May;69(5):540. doi: 10.1016/j.annemergmed.2017.03.051. PMID: 25533140.
- Chrimes N, Higgs A, Hagberg CA, Baker PA, Cooper RM, Greif R, Kovacs G, Law JA, Marshall SD, Myatra SN, O’Sullivan EP, Rosenblatt WH, Ross CH, Sakles JC, Sorbello M, Cook TM. Preventing unrecognised oesophageal intubation: a consensus guideline from the Project for Universal Management of Airways and international airway societies. Anaesthesia. 2022 Dec;77(12):1395-1415. doi: 10.1111/anae.15817. Epub 2022 Aug 17. PMID: 35977431; PMCID: PMC9804892.
- Cook TM, Woodall N, Harper J, Benger J; Fourth National Audit Project. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 2: intensive care and emergency departments. Br J Anaesth. 2011 May;106(5):632-42. doi: 10.1093/bja/aer059. Epub 2011 Mar 29. PMID: 21447489.
- Hansel J, Law JA, Chrimes N, Higgs A, Cook TM. Clinical tests for confirming tracheal intubation or excluding oesophageal intubation: a diagnostic test accuracy systematic review and meta-analysis. Anaesthesia. 2023 Aug;78(8):1020-1030. doi: 10.1111/anae.16059. Epub 2023 Jun 16. PMID: 37325847.
- Kovacs G, Duggan LV, Brindley PG. Glottic impersonation. Can J Anaesth. 2017 Mar;64(3):320. doi: 10.1007/s12630-016-0804-x. Epub 2016 Dec 27. PMID: 28028675.
- Mort TC. Esophageal intubation with indirect clinical tests during emergency tracheal intubation: a report on patient morbidity. J Clin Anesth. 2005 Jun;17(4):255-62. doi: 10.1016/j.jclinane.2005.02.004. PMID: 15950848.
- Russotto V, Myatra SN, Laffey JG, Tassistro E, Antolini L, Bauer P, Lascarrou JB, Szuldrzynski K, Camporota L, Pelosi P, Sorbello M, Higgs A, Greif R, Putensen C, Agvald-Öhman C, Chalkias A, Bokums K, Brewster D, Rossi E, Fumagalli R, Pesenti A, Foti G, Bellani G; INTUBE Study Investigators. Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients From 29 Countries. JAMA. 2021 Mar 23;325(12):1164-1172. doi: 10.1001/jama.2021.1727. Erratum in: JAMA. 2021 Jun 22;325(24):2507. doi: 10.1001/jama.2021.9012. PMID: 33755076; PMCID: PMC7988368.
- Sakles JC, Ross C, Kovacs G. Preventing unrecognized esophageal intubation in the emergency department. J Am Coll Emerg Physicians Open. 2023 Apr 29;4(3):e12951. doi: 10.1002/emp2.12951. Erratum in: J Am Coll Emerg Physicians Open. 2023 May 30;4(3):e12986. doi: 10.1002/emp2.12986. PMID: 37128296; PMCID: PMC10148380.
FOAM and web resources
- PUMA – Preventing unrecognised oesophageal intubation (consensus guideline)
- REBEL Cast Ep99: The INTUBE Study – Adverse Peri-Intubation Events in the Critically Ill

Critical Care
Compendium
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC