
![]()
William John Adie

William John Adie (1886-1935) was an Australian neurologist.
Adie is best remembered for his detailed characterisation of the tonic pupil associated with areflexia (Holmes-Adie syndrome), a constellation of signs he first described in 1931 and elaborated on in 1932. Although earlier reports of similar pupillary abnormalities existed, Adie’s distinction lay in his emphasis on the benign nature of the disorder and its separation from neurosyphilitic conditions such as the Argyll Robertson pupil.
Adie contributed significantly to the clinical understanding of narcolepsy. His 1926 paper in Brain, Idiopathic narcolepsy: a disease sui generis, was one of the earliest to consolidate the disorder into a distinct nosological entity. His discussion of sleep mechanisms and case-based clinical analysis helped demarcate narcolepsy from related disorders such as epilepsy and idiopathic hypersomnia.
Adie’s additional publications addressed a broad range of neurological conditions, including pituitary tumours, multiple sclerosis, dystrophia myotonica, familial periodic paralysis, and hepato-lenticular degeneration. He co-authored the neurology section of Price’s Textbook of Practical Medicine with James Collier (1870–1935), a text considered among the finest general accounts of neurology of its time.
Biography
- Born October 31, 1886 in Geelong, Victoria, Australia, eldest son of David Adie
- 1899 – Left school at age 13 after his father’s death to support his family
- 1906 – Encouraged by Dr Arthur South and employer to pursue education; funded through evening classes. At age 20, travelled to the UK with a £19 one-way ticket from his uncle in Boston
- 1911 – Graduated MB ChB from the University of Edinburgh; awarded McCosh Graduate Scholarship
- 1911–1912 – Postgraduate study in Boston and New York (4 months), then in Berlin, Munich, Vienna, Paris. Appointed house physician at the National Hospital for the Paralysed and Epileptic, Queen Square, London
- 1914 – At WWI outbreak, joined 1st Northamptonshire Regiment as medical officer; survived retreat from Mons due to coincidental measles. Transferred to Leicestershire Regiment; saw extensive action in France
- 1916 – Mentioned in despatches for saving soldiers during gas attack using improvised urine-soaked masks. Took charge of 7th General Hospital; consultant in management of head injuries; married Lorraine Bonar of Edinburgh (two children). Appointed medical registrar at Charing Cross Hospital, London
- 1918 – Co-authored statistical report on 656 head injuries with Wagstaffe
- 1919 – Admitted MRCP (London)
- 1925 – Elected FRCP; awarded gold medal for MD thesis on idiopathic narcolepsy, University of Edinburgh
- 1926 – Published influential paper: Idiopathic narcolepsy: a disease sui generis in Brain
- 1927 – Co-authored paper with Macdonald Critchley on frontal lobe signs: “forced grasping and groping”
- 1929 – Secretary, Section of Neurology and Psychological Medicine, British Medical Association annual meeting
- 1931 – Described tonic pupil with areflexia (pseudo-Argyll Robertson pupil) in British Medical Journal
- 1932 – Expanded on the syndrome in Brain, defining clinical forms; term “Adie syndrome” became established; co-founded Association of British Neurologists at meeting in the home of Gordon Morgan Holmes
- 1932 – First signs of angina pectoris
- 1935 – Resigned from clinical duties due to worsening health
- Died March 17, 1935 in Golders Green, London, of myocardial infarction aged 48
He was honoured in his hometown of Geelong, Australia in a long obituary entitled “Geelong boy who made good in London” published in the Geelong Advertiser
Medical Eponyms
Adie Syndrome (1931)
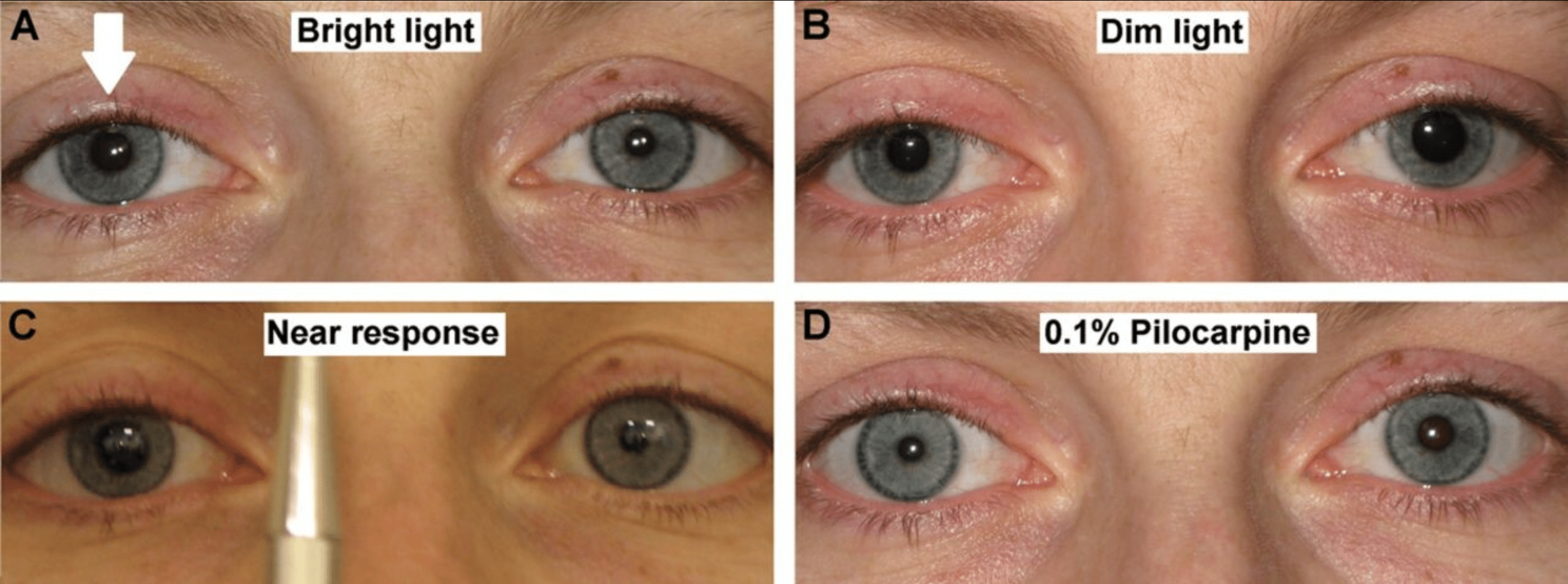
Holmes-Adie syndrome (Adie syndrome) is a benign, typically unilateral neurological condition characterised by a tonic pupil, light–near dissociation, and absent deep tendon reflexes.
It results from postganglionic parasympathetic denervation, most commonly at the level of the ciliary ganglion, and may also affect autonomic fibres to spinal reflex arcs.
Unilateral tonic pupil is more common in women, often presenting in early adulthood. While typically idiopathic, associations with viral or bacterial illness, trauma, or autoimmune disorders have been documented.
1931 – Adie described six cases of patients (five women) with tonic pupils and areflexia, without evidence of syphilis in Pseudo-Argyll Robertson Pupils with Absent Tendon Reflexes: A Benign Disorder Simulating Tabes Dorsalis. Adie emphasised the benign nature of the disorder and its frequent misdiagnosis as neurosyphilis
I wish to draw attention to a benign symptomless disorder characterized by pupils which react on accommodation but not to light, and by absent tendon reflexes…Though harmless in itself it merits recognition because it is often mistaken for a manifestation of syphilis of the nervous system, with unfortunate consequences…
Adie, May 1931
Adie recognised the work of his colleagues including Symonds, Holmes, Markus and Robert Foster Moore (1878-1963) who later expressed his ‘dissatisfaction’ at not having been ascribed the eponym…
Note – After this was written, Mr. Foster Moore kindly allowed me to read the typescript of his paper on the non-luetic Argyll Robertson pupil, which he read at the recent ophthalmological congress. In one of his fifteen patients with this abnormal reaction of the pupil, the knee-jerks were absent: in another they were obtained with reinforcement only.
1931 – Gordon Morgan Holmes identified 19 patients with myotonic pupils and presented his paper Partial iridoplegia to the Ophthalmological Society of the United Kingdom
By very slow contraction on convergence, and even slower relaxation. The reflex to light is often lost too. One or both eyes may be affected.… In the present state of our knowledge a separation of those cases in which the tendon jerks are absent from those in which they persist is unjustifiable…the similarity of the symptoms in all these cases naturally suggests a common aetiology.
Holmes, 1931
1932 – Adie publishes a definitive review of tonic pupils and absent reflexes, formally describing the syndrome as “a benign disorder sui generis.” In Tonic pupils and absent tendon reflexes, Adie consolidated his clinical observations with long-term follow-up. He presented 19 personal cases and reviewed 45 others from literature, noting that many had been misdiagnosed with tabes dorsalis.
This benign disorder, sui generis, seems to me to be distinct from all known organic diseases of the nervous system… it does not progress, has no grave underlying cause, and does not indicate syphilis.
Adie, 1932
Adie-Critchley syndrome (1927)
A phenomenon caused by tumour of the contralateral frontal lobe superior part of area 6. When an object is placed in one hand of a patient, they grasp it and hold it tightly. If attempots are made to withdraw the object, the grip tightens, and the patient is unable to voluntarily relax their grip to release the object.
Adie and MacDonald Critchley (1900-1997) describe three cases of frontal tumours, in each of which there was marked involuntary grasping and groping movements in the contralateral limb caused by a tumour in the upper and posterior part of the frontal lobes. Attention is drawn to the resemblance in the infant of 3-18 months, whose grasping and groping is not under voluntary control. When the parts of the cortex which subserve the conditioned reflexes are damaged then the unconditioned, less controlled reactions appear.
The movements in the flexors and extensors of the forearm and hand are co-ordinated perfectly so long as the movements are gentle and the hand is empty; yet certain movements of the hand cannot be prevented, and once the hand has closed reflexly upon an object, or has been closed voluntarily and firmly, it cannot be opened. The will to open it is there; the extensors are innervated powerfully but the flexors fail to relax. Relaxation is delayed, and the grip tightens when attempts are made to remove an object from the hand passively and when the patient makes voluntary efforts to relax ; partial or complete relaxation occurs when voluntary innervation ceases, and when the palm is no longer stimulated.
Adie, Critchley 1927
Note: In 1926, John Farquhar Fulton (1899-1960) published his doctoral thesis on Muscular Contraction and the Reflex Control of Movement in which he first described the concept of the Adie-Critchley phenomenon.
Key Medical Contributions
Narcolepsy (1926)
In Brain (1926), Adie published Idiopathic narcolepsy: a disease sui generis, a landmark clinical essay that distinguished narcolepsy from epilepsy and other episodic disorders. He outlined core features such as daytime sleepiness, cataplexy, and hypnagogic phenomena. His work was pivotal in early efforts to classify sleep disorders neurologically.
Other Contributions
Adie published on a wide range of neurological conditions including pituitary tumours, multiple sclerosis, myasthenia gravis, dystrophia myotonica, familial periodic paralysis, and Wilson’s disease. He co-authored the neurology section in Price’s Textbook of Practical Medicine with James Collier, regarded as one of the most comprehensive neurology texts of the period.
Major Publications
- Adie WJ. Pseudo-Argyll Robertson pupils with absent tendon reflexes. A benign disorder simulating tabes dorsalis. Br Med J. 1931 May 30;1(3673):928-30
- Adie WJ. Argyll Robertson pupils true and false. Br Med J. 1931 Jul 25;2(3681):136-8.
- Adie WJ. Tonic pupils and absent tendon reflexes: a benign disorder sui generis; its complete and incomplete forms. Brain 1932;55:98–113
- Adie WJ. Complete and incomplete forms of the benign disorder characterised by tonic pupils and absent tendon reflexes. Br J Ophthalmol. 1932 Aug;16(8):449-61.
- Adie WJ, Critchley M. Forced grapsing and groping. Brain 1927; 50: 142-70.
- Adie WJ. Idiopathic narcolepsy: a disease sui generis: with remarks on the mechanism of sleep. Brain 1926; 49: 275–306.
- Adie WJ, Wagstaffe WW. A note on a series of 656 cases of gunshot wound of the head, with a statistical consideration of the results obtained. Medical Research Committee Statistical Reports, no. 1. London: Stationery Office, 1918
References
Biography
- Obituary: William John Adie. Br Med J. 1935 March 23;1(3872):624-5
- Obituary: William John Adie, M.D. Edin., F.R.C.P. Lond. Lancet 1935; 225:5821; 717.
- Beighton P, Beighton G. Adie, William John. The Person Behind the Syndrome. Springer 1997: 4-5
- Pearce JMS. William John Adie (1886–1935). J Neurol Neurosurg Psychiatry 2004; 75: 1111
- Pearce JMS. William John Adie (1886–1935). Hektoen International
- Siddiqui AA, Clarke JC, Grzybowski A. William John Adie: the man behind the syndrome. Clin Exp Ophthalmol. 2014 Nov;42(8):778-84.
- William John Adie. Inspiring physicians. RCP
Eponymous terms
- Holmes G. Partial iridoplegia associated with symptoms of other diseases of the nervous system. Transactions of the Ophthalmological Society of the United Kingdom 1931; 51: 209-28
- Brody IA, Wilkins RH. Neurology classics VII – Adie’s Syndrome. Arch Neurol. 1968;18(6):710-715.
- Wakerley BR, Tan MH, Turner MR. Teaching video neuroimages: acute Adie syndrome. Neurology. 2012 Sep 11;79(11):e97.
Eponym
the person behind the name

MD (The University of Notre Dame, Australia). Doctor at Sir Charles Gairdner Hospital, Perth, Western Australia. Interested in critical care medicine, paediatrics, ENT and ophthalmology.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |