
![]()
CICM SAQ 2011.1 Q6
Questions
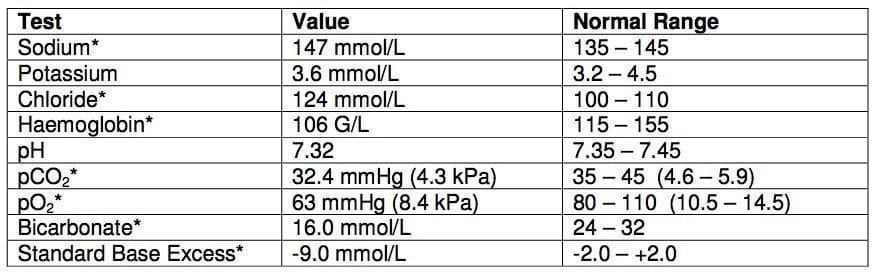
6.1. This blood gas report was taken from a lady hospitalised for recurrent urinary tract infections. She was transferred to the ICU because of nosocomial pneumonia.

- a) Comment on the acid-base status.
- b) List 2 likely causes of the acid-base derangement in this patient.
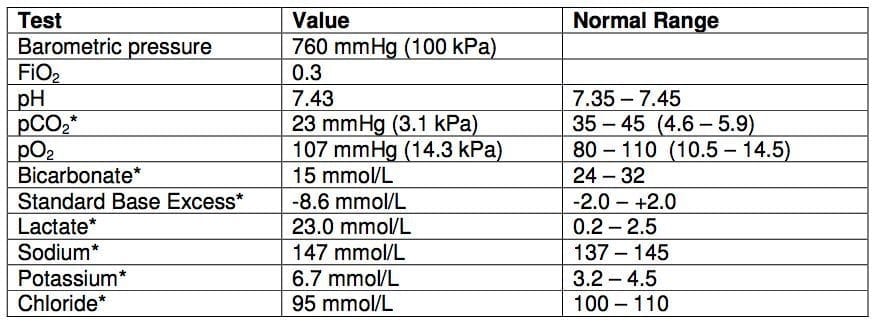
6.2. A 40 year old 70 kg male has gram negative sepsis and has developed bilateral pulmonary infiltrates. The following are data from blood gas analysis.

- a) Could this blood gas be consistent with the definition of acute respiratory distress syndrome (ARDS)? Give your reasoning.
- b) What dose of sodium bicarbonate (in mmol) would be required to reverse the metabolic acidosis? Show your calculation method.
6.3. Following laparotomy for haemoperitoneum, a patient is transferred to ICU. Blood biochemistry and arterial blood gas analysis on admission to ICU are as follows:
- a) Describe the acid-base status.
- b) What is the likely cause of this disturbance?
- c) What is the underlying biochemical mechanism?
6.4. A 33 year old female has gram negative bacteraemia and septic shock. The following are data from blood gas analysis.
- a) List the acid-base abnormalities.
Answers
Answer and interpretation
6.1. a) Comment on the acid-base status.
- Mixed respiratory and metabolic alkalosis
6.1. b) List 2 likely causes of the acid-base derangement in this patient.
- Respiratory alkalosis from the hyperventilation due to the pneumonia
- Metabolic alkalosis from vomiting or diuretic use.
6.2. a) Could this blood gas be consistent with the definition of acute respiratory distress syndrome (ARDS)? Give your reasoning.
- No. The P/F ratio is 220.
- By definition, the problem would be acute lung injury rather that ARDS at this stage.
6.2. b) What dose of sodium bicarbonate (in mmol) would be required to reverse the metabolic acidosis? Show your calculation method.
- Dose sodium bicarbonate = Wt (kg) x 0.3 x -SBE = 70 x 0.3 x 10 = 210 mmol
6.3. a) Describe the acid-base status.
- Normal anion gap metabolic acidosis with appropriate respiratory compensation
6.3. b) What is the likely cause of this disturbance?
- Resuscitation with large volume saline infusion.
6.3. c) What is the underlying biochemical mechanism?
- ECF dilution by fluid with strong ion difference of zero
6.4. a) List the acid-base abnormalities.
- Lactic acidosis
- Anion gap elevation (37 mEq/L)
- Metabolic alkalosis
- Respiratory alkalosis
- Pass rate: 86.1%
- Highest mark: 9.25

Examination Library
CICM
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC