![]()
A Subtle Sign of Something Sinister
aka ECG Exigency 007
A 65-year old man presents to ED at 1am with 90 minutes of central chest pressure that awoke him from sleep. He says he thinks he has ‘indigestion’. The pain is non-radiating, with mild shortness of breath, but no nausea, vomiting or diaphoresis. He is an ex-smoker with a 20 pack-year history. There is no previous history of IHD, diabetes, hypertension or high cholesterol.
On arrival he looks well, with normal heart rate (54 bpm), blood pressure (127/86) and oxygen saturations (98% on room air). His pain has improved slightly with sublingual nitrates in the ambulance, although he still has some ongoing chest discomfort.
His ECG is shown below:

Questions
Q1. Can you describe the ECG?
Answer and Interpretation
The ECG shows:
- Sinus rhythm at 54 bpm
- Normal axis
- Normal intervals
- Borderline left atrial enlargement with a bifid P wave in lead II (P mitrale) and enlargement of the terminal negative portion of the P wave in V1
- Essentially normal ST segments and T waves, except for some non-specific T-wave flattening in aVL
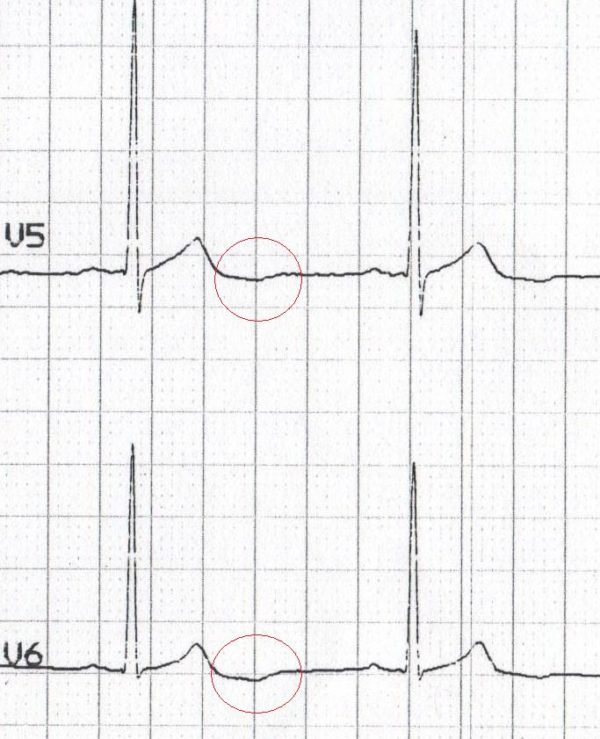
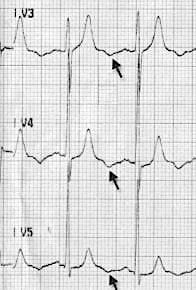
- Inverted U waves in the lateral leads I, V5 and V6 (and possibly also in leads II and III)
Q2. What is the significance of these ECG findings?
Answer and Interpretation
Most important finding: inverted U waves in the lateral leads
In patients presenting with chest pain, inverted U waves:
- Are a very specific sign of myocardial ischaemia
- May be the earliest marker of unstable angina and evolving myocardial infarction
- May be observed during attacks of Prinzmetal angina
- Have been associated with LAD or LMCA occlusion and the presence of left ventricular dysfunction
- U wave inversion tends to occur mainly in the lateral leads (I, aVL, V5-6) and may be seen either during ischaemic symptoms or at rest.
With this patient’s history, the U wave inversion would be strongly suggestive of an acute coronary syndrome (unstable angina or NSTEMI).
Inverted U waves may also be seen in:
- Hypertension
- Valvular heart disease
- Congenital heart disease
- Cardiomyopathy
- Hyperthyroidism

Q3. How would you manage this patient?
Answer and Interpretation
- This patient needs to be managed as a suspected acute coronary syndrome with analgesia, nitrates, aspirin, clopidogrel +/- low-molecular-weight heparin (enoxaparin)
- At this stage there are no indications for thrombolysis or emergent PCI
- He will need serial ECGs and troponins to look for evidence of infarction
- He needs to be admitted under a cardiology team to a monitored bed for further investigation (e.g. angiography
Q4. Can you guess what happened next?
Answer and Interpretation
- This was a difficult case to sell to cardiology, as the initial troponin I was equivocal (0.05 ng/mL at 2 hours) and the cardiology registrar was dubious about the significance of the ECG changes
- The patient ended up spending the night in ED in a monitored bed
- Serial cardiac enzymes confirmed a NSTEMI, with a troponin I of 0.87 ng/mL at 6 hours and 4.0 ng/mL at 12 hours
- Serial ECGs remained unchanged throughout his hospital stay – the lateral U wave inversion persisted and there was no progression to ST segment elevation or depression
- In the morning, he was transferred to a CCU bed under the care of a cardiologist, with angiography planned for the following day
Further reading
Related topics
- LITFL: ECG Library – U wave
References
- Gerson MC, McHenry PL. Resting U wave inversion as a marker of stenosis of the left anterior descending coronary artery. Am J Med. 1980 Oct;69(4):545-50.
- Girish MP, Gupta MD, Mukhopadhyay S, Yusuf J, Sunil Roy TN, Trehan V. U wave: an important noninvasive electrocardiographic diagnostic marker. Indian Pacing Electrophysiol J. 2005 Jan 1;5(1):63-5.
- Pérez Riera AR, Ferreira C, Filho CF, Ferreira M, Meneghini A, Uchida AH, Schapachnik E, Dubner S, Zhang L. The enigmatic sixth wave of the electrocardiogram: the U wave. Cardiol J. 2008;15(5):408-21.
- Sovari AA, Farokhi F, Kocheril AG. Inverted U wave, a specific electrocardiographic sign of cardiac ischemia. Am J Emerg Med. 2007 Feb;25(2):235-7.
- Nagayoshi et al. Inverted U-wave and myocardial ischaemia. QJM: An International Journal of Medicine, Issue 7, July 2018, Page 493.
- Hampton, JR. The ECG In Practice, 6e
- Mattu A, Brady W. ECG’s for the Emergency Physician 1
- Mattu A, Brady W. ECGs for the Emergency Physician 2
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric, 6e
- Wagner, GS. Marriott’s Practical Electrocardiography 12e
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF

CLINICAL CASES
ECG EXIGENCY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.