
![]()
Are you Satisficed?
aka To Err is human 002
At handover in ICU, a junior resident mentions that an intubated and ventilated 68 year-old man, who had cardiac surgery 4 days previously, has developed an increasing FiO2 requirement over the course of the day. He says this is explained by a new left lower zone opacity that was seen on the patient’s chest radiograph in the morning. Antibiotics were started for a hospital acquired pneumonia.
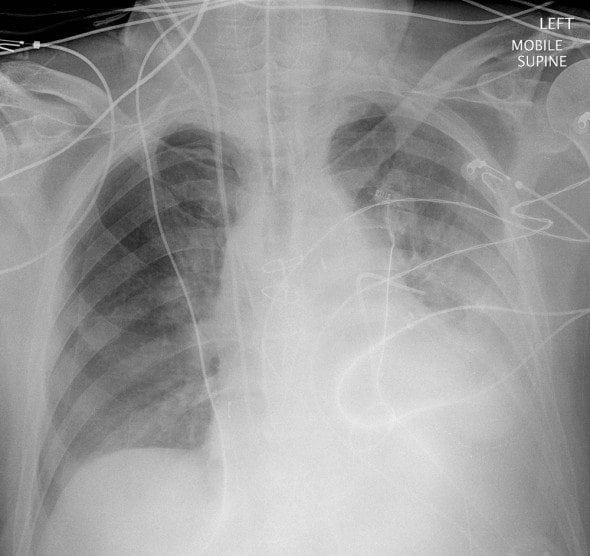
After handover is finished you review the patient’s chest x-ray taken in the morning:
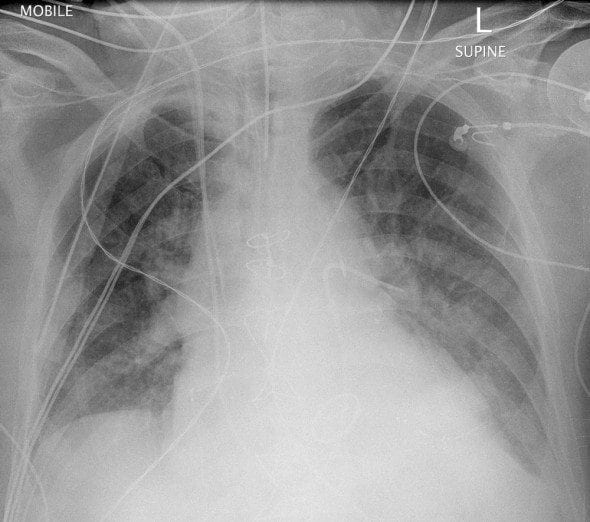
..and compare it to his previous chest film, taken the day before:
Questions
Q1. What are the chest radiograph findings?
Answer and interpretation
Your colleague was correct, there is a new left lower zone opacity. This could represent consolidation, collapse and/or an effusion. This finding would contribute to an increased FiO2 requirement.
Numerous other chest radiograph findings are unchanged — they include:
- sternal wires
- cardiomegaly
- bilateral alveolar opacities and prominent upper lobe vessels consistent with pulmonary edema
- a replaced mitral valve
- various equipment:
a correctly positioned endotracheal tube, a pulmonary artery catheter, an internal jugular vein central venous catheter, pacing wires and a tangle of other monitoring leads.
However, there is also one important new finding: the development of a right-sided pneumothorax. Most likely this has enlarged over the course of the day as a result of positive pressure ventilation, and is probably a major factor contributing to the patient’s increasing oxygen requirements.
Q2. What cognitive bias or heuristic can lead to abnormalities being missed in a situation like this?
Answer and interpretation
This heuristic (a cognitive “rule of thumb” or short-cut) causes us to stop searching for further findings once one abnormality has been found. It is a universal human tendency. The term ‘satisficing‘ was coined by Nobel prize-winning economist and polymath Herbert Simon and is a hybrid of ‘satisfying’ and ‘sufficing’.
In the absence of the left lower zone opacity the resident probably would have searched harder for another cause of the increasing oxygen requirement. By finding an obvious abnormality that potentially explained the deterioration his ‘search satisficing’ needs were fulfilled.
‘Search satisficing’ is a type of premature closure, which describes the more general tendency to end a decision-making process early, before the decision has been completely verified.
‘When the diagnosis is made, the thinking stops’.
Q3. What are some other situations where this cognitive bias or heuristic may be important?
Answer and interpretation
The possibilities are nearly endless in medicine.
Some classic examples include:
- Co-ingestants in drug overdoses
— the unconscious patient brought in with an empty pack of diazepam — maybe the paramedics didn’t find the the empty pack of amitriptyline under the bed?
[Check out this Poison Review example of premature closure almost leading to trouble] - Removing foreign bodies from wounds
— the euphoria of finally extracting a hard-won foreign body can easily distract from the need to search for more. - Trauma patients with spine injuries
— there may be multiple injuries at multiple levels, particularly when it comes to C-spine fractures. - Fall from a height with heel pain
— the calcaneal fracture may be obvious, but what about the associated pelvis or spine fractures? - Injuries to ring structures
— injuries to so-called ‘ring structures’ (such as the pelvis, mandible or ankle) typically fracture in more than one place.
Leave a comment if you can think of other important situations where ‘search satisficing’ may lead to errors.
Q4. How can this cognitive bias or heuristic be avoided?
Answer and interpretation
Some ways to avoid making errors due to ‘search satisficing’ are to:
- Use metacognition (‘think about thinking’)
— be aware of our universal tendency to ‘search satisfice’ and know when it is likely to be important. - Be systematic in the situations when it is likely to occur
— don’t rush or take short-cuts. That’s one reason why ‘tertiary surveys’ are so important in trauma patients. - Use checklists
— an example is the standardised trauma sheet used in many hospitals.
— make the statement, “there is, or is not, a pneumothorax present”, a routine part of CXR interpretation. - Ask yourself: “Could there be something else going on?”
— this is especially important if the patient continues to deteriorate despite treatment. - ‘Phone a friend’
— get a second opinion if available, doctors always like to find stuff that their colleagues have overlooked!
[see the role of the consultant]
Q5. Why does this cognitive bias or heuristic exist?
Answer and interpretation
In general cognitive biases and heuristics probably exist because they conferred an evolutionary advantage to our ancestors (error management theory), or because of ‘bounded rationality‘.
From the error management theory perspective, ‘search satisficing’ may have been a useful survival strategy for hunter-gathers, in that ‘a bird in the hand is worth two in the bush’. According to the theory of bounded rationality, our ability to reason is limited by:
- the information available,
- our cognitive abilities, and
- the limited time we have to make decisions.In situations where a fully optimized reasoning process is simply not feasible due to the above limitations, we use heuristics instead. Such heuristics are useful because they work most of the time… but it is inevitable that they will sometimes lead to mistakes.
References
- Weingart S, Wyer P. Emergency Medicine Decision Making: Critical Choices in Chaotic Environments. McGraw-Hill
- Crosskerry P, Cosby KS, Schenkel SM, Wears RL. Patient Safety in Emergency Medicine. Lippincott Williams & Wilkins

CLINICAL CASES
to err is human
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC