
![]()
Axillary Nerve Lesions
The Axillary nerve is most commonly injured by trauma to the surgical neck of the humerus or anterior shoulder dislocations.
Axillary nerve lesions are characterized predominantly by:
- Shoulder abduction impairment:
- The deltoid abducts the arm to 90 degrees.
- Anterior fibers: flex and medially rotate the shoulder.
- Posterior fibers: extend and laterally rotate the shoulder.
- Teres minor: laterally rotates the shoulder.
- Variable anaesthesia over the region of the lower half of the deltoid muscle.
The nerve is most commonly injured by trauma to the surgical neck of the humerus or anterior shoulder dislocations.
Anatomy
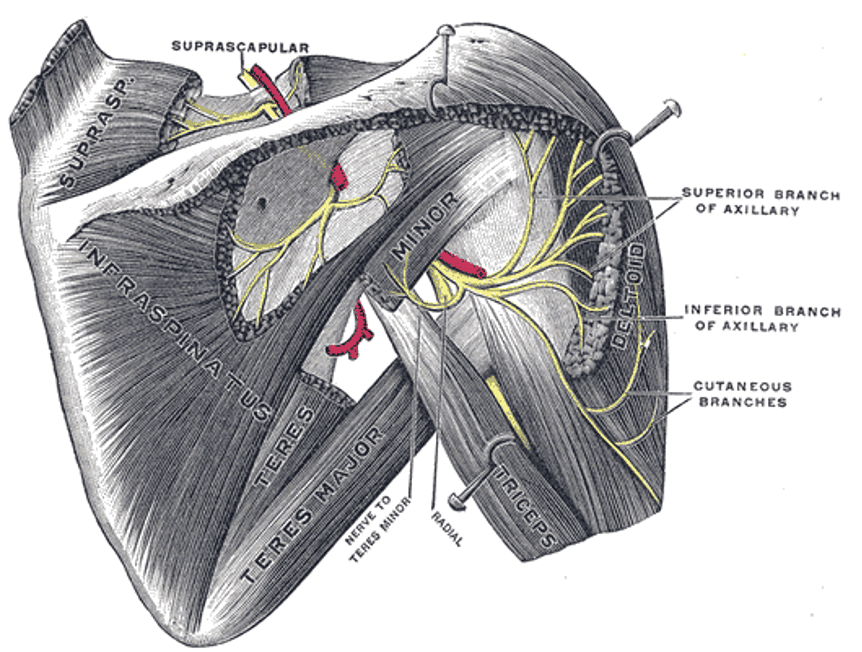
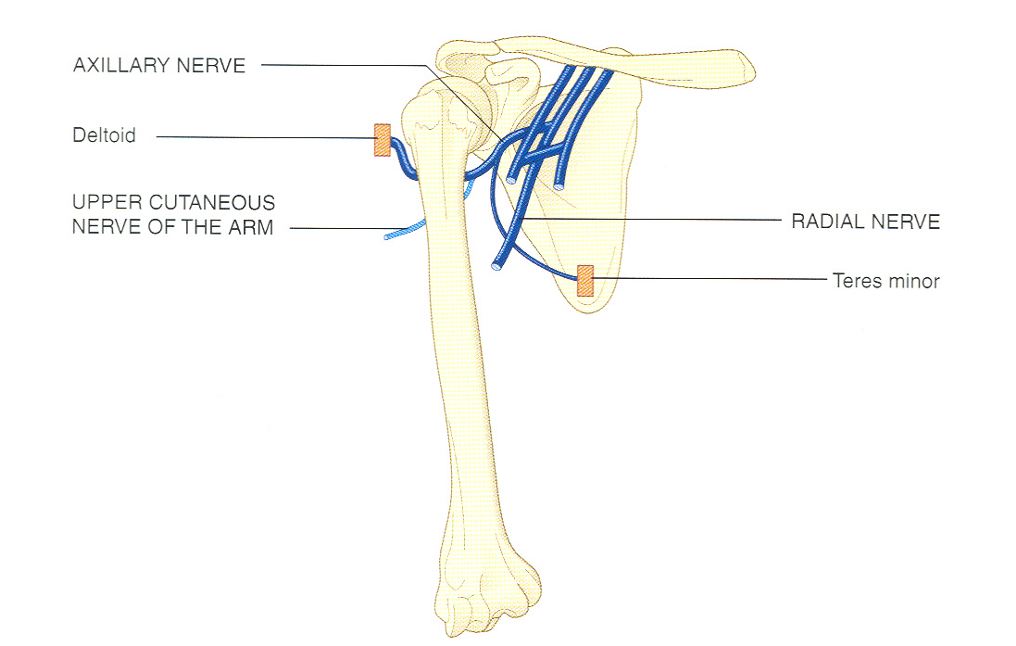
Course of the Axillary Nerve
- Originates from C5, C6 nerve roots.
- Arises from the posterior cord of the brachial plexus at the axilla, posterior to the coracoid process.
- Crosses the inferolateral surface of the subscapularis muscle.
- Passes through the quadrilateral space beneath teres minor with the posterior circumflex humeral artery.
- Travels around the posterior and lateral humerus, deep to the deltoid, and divides into anterior and posterior branches.
Innervations
Anterior branch:
- Middle and anterior deltoid.
Posterior branch:
- Teres minor.
- Posterior deltoid.
- Superior lateral brachial cutaneous nerve.
Actions of Innervated Muscles
Deltoid muscle:
- Main abductor of the shoulder (middle fibers).
- Anterior fibers: flexion and medial rotation.
- Posterior fibers: extension and lateral rotation.
Teres minor:
- Lateral rotation and stabilization of the shoulder joint.
Pathology
Causes
- Trauma:
- Direct trauma to surgical neck of the humerus.
- Surgical injury (e.g. rotator cuff surgery).
- Neuropraxias:
- Anterior shoulder dislocations compressing the nerve in the quadrilateral space.
- Improper use of crutches pressing into the axilla.
- Mass lesions:
- Tumours.
- Abscesses.
- Neuropathies:
- Rarely affected by mononeuropathies.
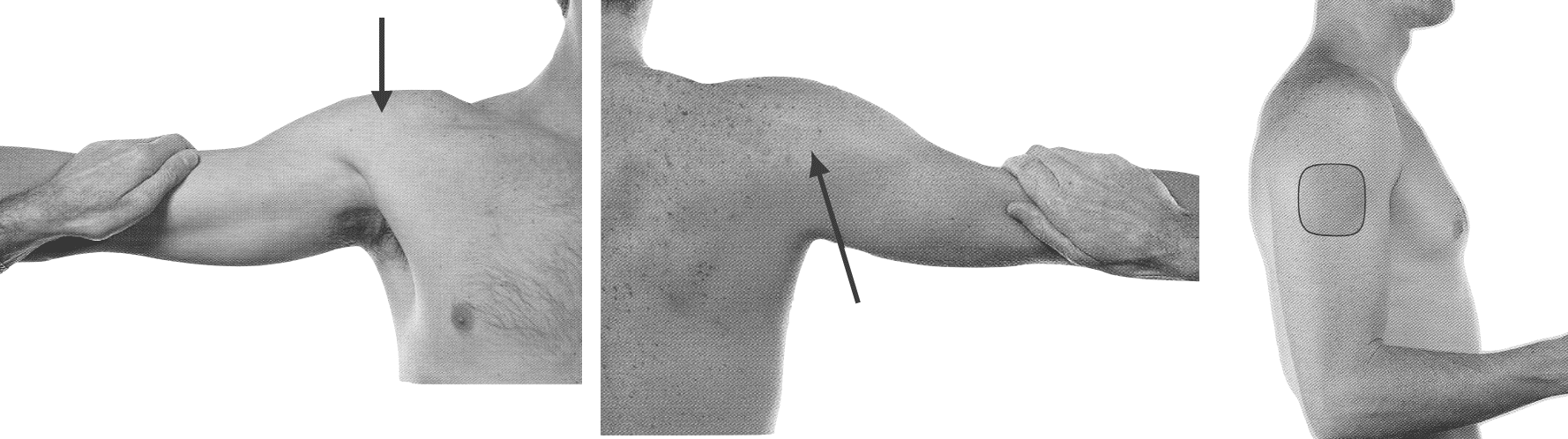
Middle: Deltoid, posterior view, (Axillary nerve, C5, 6). The patient retracts the abducted arm against resistance. Arrow: the posterior fibers of deltoid can be seen and felt.
Right: The approximate area, (lower ½ of deltoid muscle), where sensory changes may be found in lesions of the sensory nerve.
Axillary Nerve Deficits
Sensory:
- Loss over the lower half of the deltoid.
Motor:
- Deltoid wasting; palpable greater tuberosity.
- Marked abduction weakness (spared supraspinatus activity via suprascapular nerve).
- Teres minor paralysis is usually clinically silent.
Investigations
When to investigate
- Unclear diagnosis or to rule out systemic pathology.
Nerve conduction studies
- For diagnosis, rule out generalised disease, and assess prognosis.
Blood tests
Consider depending on suspicion:
- FBC
- U&Es/glucose
- CRP
- ESR
- Others (e.g. lead levels)
Imaging
CT scan:
- For suspected mass lesions compressing the nerve.
MRI:
- Best for visualizing soft tissues, the nerve, and spinal cord lesions at C5-6.
Biopsy
- Rarely indicated.
- Consider in mononeuritis or suspected leprosy.
Management
General principles
- Treat the underlying cause.
- Neuropraxia:
- Reduce anterior shoulder dislocations.
- Occupational therapy:
- Splints and supportive devices.
- Physiotherapy:
- Rehabilitation or prevention of complications.
Disposition
Depends on:
- Cause of the lesion.
- Severity of symptoms.
- Acuteness of onset.
Appendix 1
Axillary Nerve Anatomy
Appendix 2
References
Publications
- Brazis PW, Masdeu JC, Biller J. Localization in Clinical Neurology. 8e 2021
- Fuller G. Neurological Examination Made Easy. 6e 2019
- O’Brien M. Aids to the Examination of the Peripheral Nervous System. 6e 2023
FOAMed
- Coni R. Neuro 101: Peripheral Nervous System. LITFL
- Nickson C. Myotomes and Differentiating Nerve Lesions. LITFL
Fellowship Notes

MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner

Educator, magister, munus exemplar, dicata in agro subitis medicina et discrimine cura | FFS |