
![]()
Can’t Intubate Can’t Oxygenate (CICO)
OVERVIEW
CICO occurs when adequate alveolar oxygen delivery cannot be achieved despite best attempts at all three upper airway rescue techniques (“Lifelines”): face mask ventilation (FMV), supraglottic airway (SGA) ventilation, and tracheal intubation (endotracheal tube, ETT).
- CICO is “can’t intubate, can’t oxygenate” (pronounced “KY-KOH”)
- Without rapid restoration of oxygenation, profound hypoxaemia, cardiac arrest, and death are inevitable.
- Definitive management is emergency front-of-neck access (FONA or eFONA) — also referred to as emergency surgical airway (ESA), surgical cricothyroidotomy, neck rescue, infraglottic rescue, or CICO rescue.
Key principles include:
- Call for help early
- Continuously reassess the effectiveness of airway rescue strategies
- Prime and prepare for FONA throughout airway management
- Maintain oxygen delivery whenever possible during airway rescue attempts
This LITFL CCC page synthesises concepts from the Vortex Approach (Chrimes, 2016), the DAS/ICS/FICM/RCA guidelines for intubation in the critically ill (Higgs et al, 2018), ANZCA documents, and other sources.
INCIDENCE OF CICO
CICO situations are rare, but are about 10 times more common in ED/ICU settings than in anaesthesia in operating rooms. This likely reflects differences in:
- Anatomical challenge -difficult anatomy (e.g.facial and airway trauma, airway obstruction, tumours, infection, obesity), airway contamination (e.g. blood, vomitus)
- Physiological challenge – rapid oxygen desaturation, haemodynamic compromise, concomitant
- Situational challenge – ad hoc teams, time-critical and information-poor scenarios, suboptimal environments and/or equipment.
Incidence in different settings:
- Operating Theatre (Anaesthesia)
- ≈0.01% (≈1 per 10,000 cases) (Cook et al, 2011 – NAP4; Waterson et al, 2014)
- ≈0.05–0.1% in obstetric anaesthesia (Kinsella et al, 2015)
- Emergency Department (ED)
- ~0.3% eFONA incidence (Alkhouri et al, 2021)
RECOGNISING CICO
The Vortex Approach provides a simple model for recognising deteriorating airway situations and determining when FONA is required. Three upper airway rescue attempts (or “Lifelines” in Vortex terminology) can restore alveolar oxygenation:
- Face mask ventilation (FMV)
- Supraglottic airway (SGA)
- Endotracheal tube (ETT)
When successful use of any of these achieves adequate alveolar oxygen delivery, the patient is in the “green zone” (Vortex terminology for adequate alveolar oxygenation) and progression to a CICO situation is averted.
Should one or more attempts at any of these three techniques fail, it is important to:
- Escalate awareness of potential progression to CICO
- Prepare for FONA in parallel with airway rescue attempts (see “Priming for FONA” below)
- Recognise that declining oxygenation and prolonged airway manipulation increase the urgency of airway rescue
- Avoid repeated unsuccessful attempts that do not meaningfully improve the likelihood of success
A CICO situation exists when adequate alveolar oxygen delivery cannot be achieved despite best efforts using the three upper airway rescue techniques (ETT, SGA, and FMV Lifelines).
PRIMING FOR FONA
“Priming for FONA” formalises preparation before a true CICO situation develops.
- Delayed transition to FONA, rather than performance of the procedure itself, is the major contributor to airway-related morbidity and mortality.
- Priming for FONA should occur simultaneously with attempts at the three upper airway rescue techniques (Lifelines) — not only once they have all failed.
- CICO Status should be escalated after an unsuccessful best effort at any upper airway rescue technique (Lifeline), or earlier if a difficult airway is anticipated or the clinical picture is deteriorating.
- Consider further escalation in CICO status if:
- Attempt at a second airway rescue technique fails
- SpO2 is rapidly declining or patient is hypoxaemic (SpO2 <90%)
- Difficult airway is predicted
- Attempt at securing the airway is prolonged
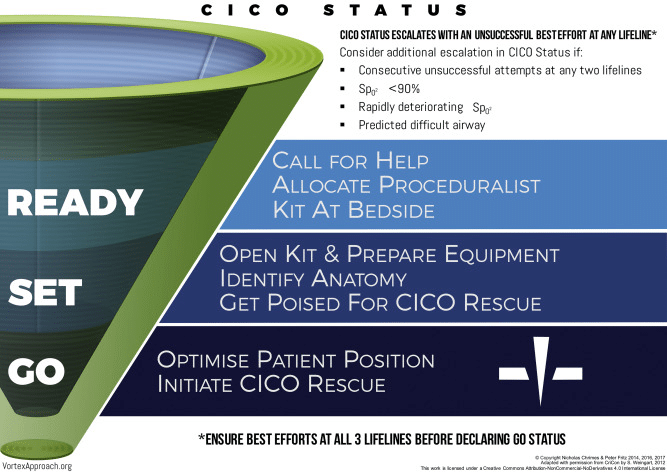
Practical approach: READY → SET → GO
- READY: Failed intubation attempt → FONA kit at bedside.
- SET: Failed rescue oxygenation via FMV or SGA → FONA kit opened and prepared.
- GO: All 3 techniques failed → CICO declared → perform FONA immediately.
This staged approach improves both psychological readiness and operational efficiency.
| CICO status | Trigger | Statement and team response | Vortex concept | DAS concept |
|---|---|---|---|---|
| READY | First failed “best” attempt at an airway rescue technique (usually ETT) | Call for help Declare: “Failed intubation” State: “Bring the FONA kit” Team confirm its location and allocates proceduralist (CICO rescuer) | Escalating CICO status; begin priming for FONA while upper airway rescue techniques (Lifelines) continue | Failed Plan A: intubation |
| SET | Failure of best attempt at a second upper airway rescue technique (FMV or SGA) | “Open the FONA kit, prepare for FONA” Team assign roles; prepare FONA equipment, identifies landmarks; anticipate imminent CICO (within 1 minute) | Approaching the centre of the Vortex; prepare for CICO Rescue | Failed one of Plan B/C: rescue oxygenation (either FMV or SGA) |
| GO | Failure of best attempt at all three upper airway rescue techniques (ETT, SGA, FMV) Explicit declaration of CICO | Declare: “This is a CICO situation, perform FONA” Optimise patient position for FONA; ensure neuromuscular blockade; CICO rescuer proceeds with FONA procedure | Commit to, and perform, CICO Rescue | Failed Plan A, B, and C Proceed to Plan D: FONA |
TRANSITION TO FONA
Emergency FONA is indicated when best attempts at:
- Intubation (ETT) have failed, and
- Rescue oxygenation using FMV and SGA have failed
Do not proceed with GO until all three upper airway rescue techniques have failed.
There is no specific oxygen saturation threshold that mandates FONA.
- The goal is to establish an emergency airway before profound hypoxaemia develops, rather than waiting until severe desaturation occurs.
- In some rare situations, senior clinicians may determine that FONA may be the preferred initial approach (e.g. awake tracheostomy for airway obstruction due to a tumour)
During transition to FONA:
- Explicitly declare:
- “This is a CICO situation, perform FONA”
- Continue attempts at oxygen delivery via nasal oxygen, FMV, or SGA if feasible
- Ensure adequate neuromuscular blockade
- Ensure optimal positioning of patient for FONA
- Avoid further repetitive attempts at upper airway rescue that delay definitive management
BEST ATTEMPTS AT UPPER AIRWAY RESCUE (“LIFELINES”)
A “best attempt” is an appropriately optimised attempt by an experienced operator using suitable equipment, positioning, adjuncts, and rescue manoeuvres.
- Repeated identical attempts are rarely helpful.
- Efforts should be limited and each attempt should involve a meaningful change intended to improve success.
- Maximum of 3 attempts at each of ETT, SGA, and FMV (Chrimes, 2016; Higgs et al, 2018)
- Some guidelines suggest even fewer attempts, e.g. ANZCA ETT x3, SGA x2, FMV x1 (Watterson et al, 2014)
- Some guidelines allow for an extra attempt if an airway expert arrives to assist
The STOPME mnemonic can be used to address 6 categories of change to optimise upper airway rescue (“Lifelines”):
- Suction/increased flow
- Tone (neuromuscular blockade)
- Operator (ensure most expert operator available)
- Positioning and adjuncts
- Manipulations/ maneuvers
- Equipment: Size/type of device
After a best attempt at an upper airway rescue technique (“Lifeline”):
- Declare this explicitly to the team
- Progress to the next upper airway rescue technique (“Lifeline”) if oxygenation has not been restored
- Continue FONA preparation throughout
Changes to consider to ensure best attempts at upper airway “lifelines” differ for each technique (see below)
Face mask ventilation (FMV)
| Change | Details |
|---|---|
| Suction/ increased flow | Suction blood, secretions, or vomitus from the oropharynx; increase FiO2/fresh gas flow; use O2 flush if available |
| Tone | Deepen anaesthesia or give/increase neuromuscular blockade — laryngospasm and masseter spasm are common, correctable causes of FMV failure |
| Operator | Hand over to the most experienced operator available; move to a two-person technique (one achieves seal + jaw thrust with both hands, second person bags) |
| Positioning and adjuncts | Sniffing position, or ramped/reverse-Trendelenburg for obese or pregnant patients; chin lift; OPA/Guedel airway; NPA (bilateral NPAs plus an OPA for a “double-adjunct” seal) |
| Manipulations/ manoeuvres | Two-handed mask hold (V-E or two-thumb “thenar eminence” technique) with jaw thrust; release excessive cricoid force if it’s distorting the airway |
| Equipment (size/type) | Correct mask size for face shape/size; different mask design if seal is poor (e.g. bearded patients); leave dentures in situ in edentulous patients |
Endotracheal intubation (ETT)
| Change | Details |
|---|---|
| Suction/ increased flow | Suction blood, secretions, or regurgitated material obscuring the glottic view |
| Tone | Ensure adequate neuromuscular blockade — inadequate relaxation is a common, remediable cause of a poor laryngoscopic view |
| Operator | Hand over to the most experienced/senior laryngoscopist — changing the operator is a legitimate “change” between attempts; recruit a skilled second operator for video-assisted flexible intubation (VAFI) |
| Positioning and adjuncts | Sniffing position, or ear-to-sternal-notch ramping in obesity; bougie or stylet |
| Manipulations/ manoeuvres | External laryngeal manipulation); dynamic head lift; two-handed laryngoscope lift; release cricoid pressure if it’s obscuring the view |
| Equipment (size/type) | Smaller tube size; different laryngoscope blade; video laryngoscopy; video-assisted flexible intubation (VAFI) using flexiscope |
Supraglottic airway (SGA)
| Change | Details |
|---|---|
| Suction/ increased flow | Suction the oropharynx of blood/secretions before insertion; suction via the drain tube (second-generation devices) after placement to confirm position |
| Tone | Ensure adequate depth of anaesthesia/relaxation — inserting “too light” is a common cause of failure (coughing, biting, laryngospasm) |
| Operator | Hand over to the most experienced operator available |
| Positioning and adjuncts | Neutral or slightly flexed head position (different from the sniffing position used for ETT); jaw thrust during insertion; introducer tool if available; laryngscope to help place; bite block |
| Manipulations/ manoeuvres | Rotational insertion technique for classic/flexible LMAs if standard midline insertion fails; full lubrication of the posterior device surface; adjust cuff inflation |
| Equipment (size/type) | Try a different size, or switch device type (e.g. first-generation LMA to second-generation gastric-access device, or vice versa) |
CORRECTABLE FACTORS TO CONSIDER DURING TRANSITION TO CICO
Before or during transition to FONA, rapidly consider potentially correctable factors for why airway rescue techniques appear to have failed.. This assessment should not delay FONA.
| Category | Consider |
|---|---|
| Equipment | Oxygen failure, blocked circuit, obstructed HME filter, blocked airway device, poor mask seal |
| Airway | Excessive cricoid force, laryngospasm, foreign body, blood, regurgitated material, severe bronchospasm |
| Physiology | Profound shock, cardiac arrest, absent pulmonary perfusion causing loss of ETCO₂ |
PERFORMING FONA
The preferred emergency airway technique is:
- Surgical cricothyroidotomy (click link for more details)
- Usually performed via a scalpel-bougie-tube approach
Advantages include:
- Rapid and reliable
- High success rate
- Familiar equipment
- Ability to confirm placement with waveform capnography
- Definitive cuffed airway
- Allows positive pressure ventilation and PEEP
- Provides some protection against aspiration
Needle/ cannula techniques (including transtracheal jet ventilation, TTJV) are not recommended as the default adult CICO rescue technique because:
- They have high failure and complication rates
- They do not provide a definitive airway
- They cannot reliably provide ventilation or PEEP in critically ill patients
- Subcutaneous emphysema may complicate subsequent surgical airway attempts
FAILED FONA
Failed FONA is a catastrophic event and is frequently associated with cardiac arrest.
Consider:
- A second attempt at airway access lower in the trachea
- Surgical or percutaneous tracheostomy by an experienced operator
- Alternative FONA techniques if appropriate expertise is present
- Ongoing resuscitation according to local cardiac arrest protocols
If an airway expert arrives, a single optimised attempt at an alternative rescue technique may be reasonable.
MANAGEMENT FOLLOWING FONA
Following successful FONA:
- Confirm tracheal placement using waveform capnography
- Suction the airway as required
- Obtain chest radiography to confirm tube position and assess for complications
- Arrange surgical review of the airway wound
- Plan conversion to a formal tracheostomy or tracheal tube when appropriate
- Assess for complications including:
- Bleeding
- Pharyngeal injury
- Oesophageal injury
- Mediastinal infection
- Document the event and create an airway alert
HUMAN FACTORS
Human factors frequently contribute to delayed FONA. Common problems include:
- Fixation on repeated intubation attempts
- Reluctance to transition to a surgical airway
- Failure to recognise deterioration
- Poor communication
- Unclear team roles
Strategies that improve performance include:
- Normalising priming for CICO
- Early declaration of CICO
- Verbal declaration of completed “best attempts”
- Closed-loop communication
- Clear role allocation
- Calling for expert assistance early
- Use of cognitive aids where available
- Training in CICO scenarios and priming for CICO
EXAMPLES OF CICO ALGORITHMS AND COGNITIVE AIDS
Clinicians should be familiar with their local guidelines and cognitive aids for airway management. Examples of useful approaches to CICO transition are shown below.
ANZCA CICO Cognitive Aid
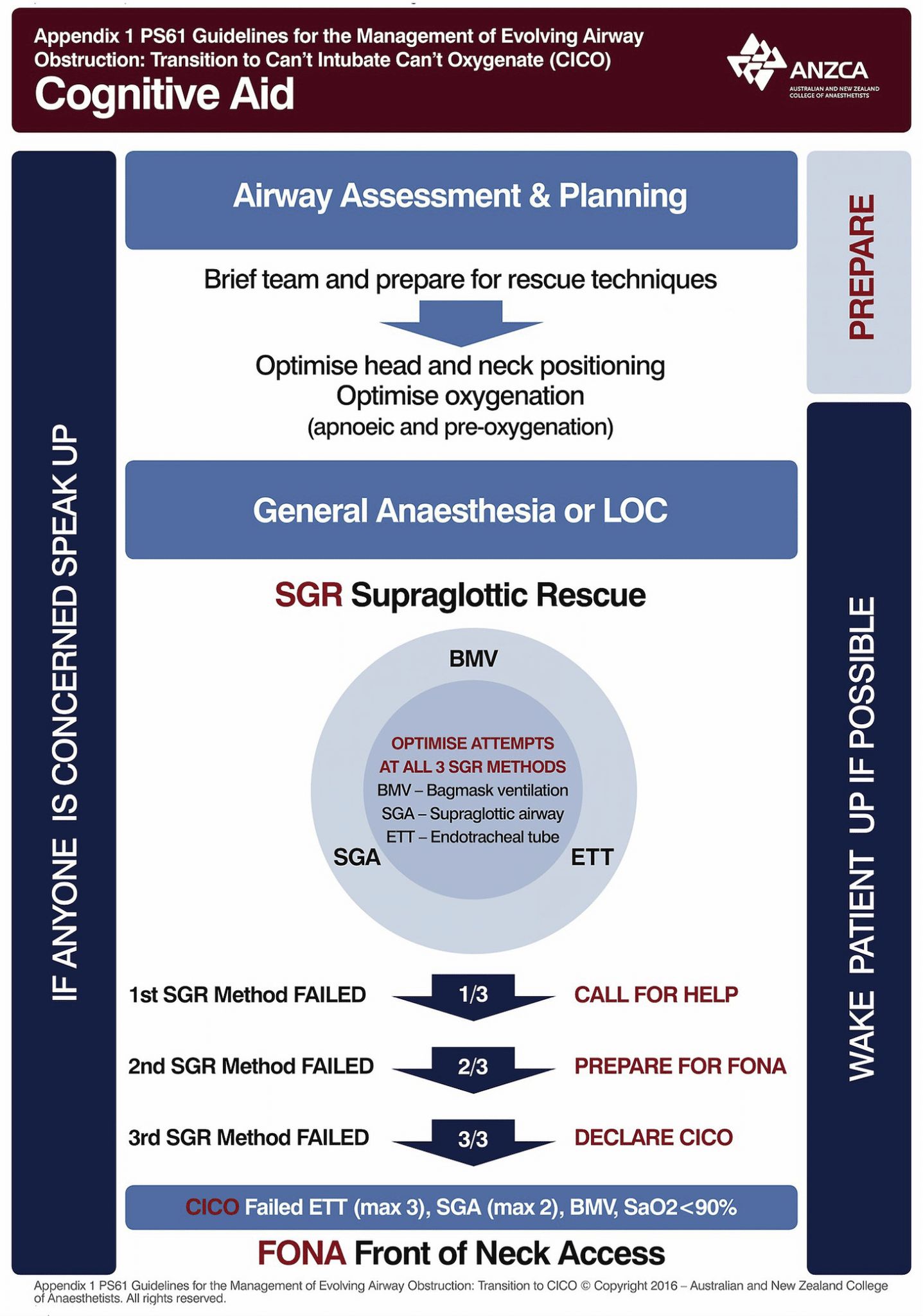
From Bradley (2020). Image source: https://www.bjanaesthesia.org/article/S0007-0912(20)30744-3/fulltext
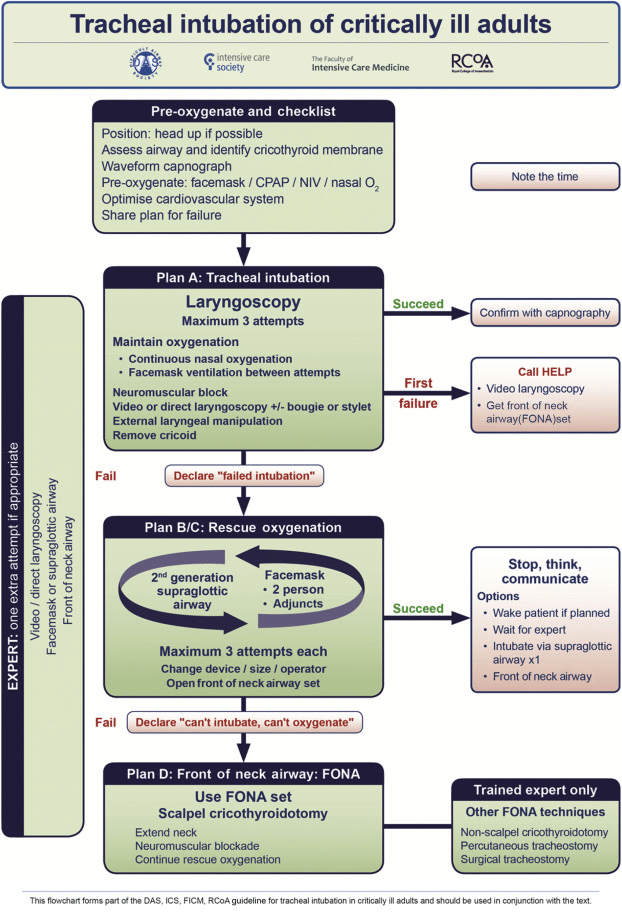
DAS/ICS/FICM/RCA Tracheal intubation of Critically Ill Adults Flowchart
Vortex CICO Status Tool
CONCLUSION
Recognise a potential CICO situation early.
- Delayed progression to FONA is a major cause of preventable harm.
- Prepare for FONA before all upper airway rescue techniques (“Lifelines”) have failed by “priming for FONA”
- Optimise each technique using meaningful changes (STOPME mnemonic) rather than repeated identical attempts.
- Explicitly declare CICO and “transition to FONA” when alveolar oxygenation cannot be achieved.
- Scalpel cricothyroidotomy is the recommended default emergency FONA rescue technique for adult CICO.
REFERENCES
LITFL
Journal articles and Guidelines
- Alkhouri H, Richards C, Miers J, Fogg T, McCarthy S. Case series and review of emergency front-of-neck surgical airways from The Australian and New Zealand Emergency Department Airway Registry. Emerg Med Australas. 2021 Jun;33(3):499-507. doi: 10.1111/1742-6723.13678. Epub 2020 Nov 11. PMID: 33179449.
- ANZCA. PG61(A) Guideline for the management of evolving airway obstruction: transition to the Can’t Intubate Can’t Oxygenate airway emergency 2017. Available at: https://www.anzca.edu.au/getContentAsset/52988fd7-b32d-4757-94c5-fa3e3dc373f6/80feb437-d24d-46b8-a858-4a2a28b9b970/PG61(A)-CICO-2017.pdf?language=en
- Bradley P. Lost in transition: use of SpO2 in the Australian and New Zealand College of Anaesthetists transition tool. Comment on Br J Anaesth 2020; 125: e38-46. Br J Anaesth. 2020 Dec;125(6):e465-e466. doi: 10.1016/j.bja.2020.09.007. Epub 2020 Oct 3. PMID: 33023737. [Fulltext article]
- Chrimes N. The Vortex: a universal ‘high-acuity implementation tool’ for emergency airway management. Br J Anaesth. 2016 Sep;117 Suppl 1:i20-i27. doi: 10.1093/bja/aew175. Epub 2016 Jul 20. PMID: 27440673. [Fulltext article]
- Chrimes N, Higgs A, Rehak A. Lost in transition: the challenges of getting airway clinicians to move from the upper airway to the neck during an airway crisis. Br J Anaesth. 2020 Jul;125(1):e38-e46. doi: 10.1016/j.bja.2020.04.052. Epub 2020 May 28. PMID: 32475685. [Fulltext article]
- Cook TM, Woodall N, Frerk C. A national survey of the impact of NAP4 on airway management practice in United Kingdom hospitals: closing the safety gap in anaesthesia, intensive care and the emergency department. Br J Anaesth. 2016 Aug;117(2):182-90. doi: 10.1093/bja/aew177. PMID: 27440629. [Fulltext article]
- Higgs A, et al; Difficult Airway Society; Intensive Care Society; Faculty of Intensive Care Medicine; Royal College of Anaesthetists. Guidelines for the management of tracheal intubation in critically ill adults. Br J Anaesth. 2018 Feb;120(2):323-352. doi: 10.1016/j.bja.2017.10.021. Epub 2017 Nov 26. PMID: 29406182. [fulltext article]
- Kinsella SM, Winton AL, Mushambi MC, Ramaswamy K, Swales H, Quinn AC, Popat M. Failed tracheal intubation during obstetric general anaesthesia: a literature review. Int J Obstet Anesth. 2015 Nov;24(4):356-74. doi: 10.1016/j.ijoa.2015.06.008. Epub 2015 Jun 30. PMID: 26303751. [fulltext article]
- Watterson L, Heard A, Marshall S. Transition from supraglottic to infraglottic rescue in the “can’t intubate can’t oxygenate” (CICO) scenario. Report from the ANZCA airway management working group. 2014. [Date accessed: July 12, 2026] Available from: http://www.anzca.edu.au/documents/report-from-the-anzca-airway-management-working-gr.pdf
FOAM and web resources

Critical Care
Compendium
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC