
![]()
Carl Westphal

Carl Friedrich Otto Westphal (1833-1890) was a German neurologist and psychiatrist.
Initially reluctant to pursue a career in neurology and psychiatry, Westphal would be inspired by Wilhelm Griesinger and go on to become one of the most prominent neuropsychiatrists of his time, publishing countless papers and editing prominent journals, training a number of world-famous neurologists including Hermann Oppenheim and Carl Wernicke, and making numerous contributions and discoveries.
A compassionate clinician, Westphal was also noted for his conscientiousness and humanity towards the sick and distinguished himself from his peers in his no-restraint approach to the care of the mentally ill. He was an earnest friend to his patient and co-workers and was highly renowned worldwide as a physician.
Westphal is eponymous with Westphal sign, Westphal syndrome, Westphall-Strümpell pseudosclerosis, Westphal-variant Huntington disease, Leyden-Westphal ataxia, and the Edinger-Westphal nucleus. He is also known for his coining of the term ‘agoraphobia’, describing the modern homosexual and describing the first case of narcolepsy and cataplexy.
Biography
- Born March 23, 1833 in Berlin to German physician Otto Carl Friedrich Westphal (1800–1879)
- 1851-1855 – Studied medicine in Berlin, Heidelberg, and Zurich
- 1855 – Doctorate from University of Berlin
- 1856 – Passed the state medical examination
- 1857 – Assistant at a smallpox department of the Berlin Charité
- 1858 – Assistant physician at the department for the mentally ill at the Berlin Charité
- 1861 – Privatdozent of psychiatry at the University of Berlin
- 1867-1868 – Pursued internal medicine after disagreements with his senior, Griesinger
- 1869 – Succeeded Griesinger as head of the department for the mentally ill at the Berlin Charité after his death; appointed associate professor
- 1870 – Described modern homosexuality in the medical literature
- 1871 – Added an outpatient clinic to his hospital, which increased his material for observation and teaching purposes
- 1872 – Coined the term ‘agoraphobia’; summarized cases of Westphal-Leyden ataxia
- 1874 – Given full professorship and appointed a Fellow of the Scientific Deputation for Medicine
- 1875 – Described Westphal’s sign and the importance of deep tendon reflexes in disease
- 1877 – Gave the first description of narcolepsy and cataplexy in the medical literature
- 1883 – Described a set of cases which would become known as Westphal-variant Huntington’s disease and Westphal-Strümpell pseudosclerosis
- 1885 – Described Westphal’s syndrome
- 1887 – Described the existence of the Edinger-Westphal nucleus in adults.
- Died January 27, 1890 in Kreuzlingen
Medical Eponyms
Leyden-Westphal Ataxia (1872)
An acute ataxia of unknown etiology, possibly secondary to an inherited disorder or a post-infectious sequela. Presents with vertigo, vomiting, proximal muscle rigidity, which can then develop into dysphasia, ataxia with convulsive seizures, dementia, and coma.
1868 – Ernst Leyden (1832-1910) first described a case of the acute ataxia in 1868.
1872 – Westphal summarized a number of observations similar to Leyden’s, which he had seen as a secondary disease to smallpox, and combine them with reference to Leyden’s first case to form a clinical picture.
German
English
C Westphal stellt als die charakteristischen Symptome dieses Krankheitsbildes folgende auf:
1. Eine eigenthümliche Sprachstörung, wobei die Sprache langsam. gedehnt, scandirend wird; die einzelnen Silben werden mit Anstrengung berausgestossen, während die Zunge selbst frei beweglich ist.
2. Ataxie der Extremitäten, bei erhaltener oder jedenfalls nicht erheblich geschwächter motorischer Kraft; dazu werden die Bewegungen öfters in einzelnen Absätzen ausgeführt und sind überhaupt verlangsamt.
3. Die Sensibilität war in allen Fällen intact.
4. Psychische Störungen wurden mehrfach beobachtet; Gemüthserregbarkeit, Gedächtnissschwäche und Dementia.
Leyden summarising Westphal’s 1872 description of the ataxia. Leyden 1891. Ueber acute Ataxie; p. 578.
C Westphal lists the following as the characteristic symptoms of this clinical picture:
1. A peculiar language disorder, with language being slow, stretched and scanned; the individual syllables are pushed out with effort, while the tongue itself is free to move.
2. Ataxia of the extremities, with preserved or at least insignificantly weakened motor strength; in addition, the movements are often performed in individual segments and are generally slowed down.
3. Sensation was intact in all cases.
4. Mental disorders were observed several times; emotional excitability, poor memory and dementia.
Leyden summarising Westphal’s 1872 description of the ataxia. Leyden 1891. Ueber acute Ataxie; p. 578.
Westphal Sign (1875)
Also known as the Erb-Westphal symptom. Refers to a decreased or absent patellar tendon reflex seen on physical exam. Initially referred to a decreased patellar reflex seen specifically in central nervous system syphilis (tabes dorsalis), but over time the eponym evolved to simply refer to the phenomena regardless of cause.
Description of deep-tendon reflexes in the medical literature dates back as early as 1863 by Jean-Martin Charcot and Alfred Vulpian.
1875 – The 1875 issue of Archiv fur Psychiatrie und Nervenkrankheiten contained adjacent papers by Wilhelm Heinrich Erb and Westphal which introduced various deep tendon reflexes and their changes in disease to the medical literature. It was for this contribution that the sign was eponymously named.
German
English
Vorkommen des ünterschenkelphänomen’s.
Die durch minimales Klopfen auf das Ligam. patellae bedingte, auf plötzlicher Contraction des Quadriceps beruhende Streckung des Unterschenkels findet sich in einer grossen Zahl der Fälle, in welchen auch die rhythmischen Fussbewegungen bei Dorsalflexion des Fusses zu beobachten sind, und zwar ebensowohl bei Hemiplegien (Hemiparesen) als bei Iähmungsartigen Zuständen beider unteren Extremitäten (Paraplegien, Paraparesen); bei ersteren pflegt die Erscheinung, wie das Fussphänomen, auf der gelähmten Seite stärker ausgeprägt vorzukommen, so dass entweder bei derselben Stärke des Reizes (des Klopfens) die Contraction des Quadriceps auf die stärker betroffene Seite stärker ist, oder ein geringerer Reiz zur Auslösung der Contraction erforderlich ist. Dasselbe giebt im Allgemeinen für die Parese beider Unterextremitäten.
Von dieser Regel finden sich indess nicht selten Ausnahmen. So kommt es bei Hemiplegien vor, dass das Unterschenkelphänomen beiderseits gleichmässig stark, das Fussphänomen nur auf der gelähmten Seite entwickelt ist, auch habe ich in einzelnen Fällen bei Fehlen des letzteren an dem gelähmten Fusse, das erstere an der gleichen gelähmten Seite vorhanden gefunden… Bei Paresen beider unteren Extremitäten ist das Unterschenkelphänomen zuweilen stark ausgeprägt… eigenthümlicher Weise (zufällig?) finden sich unter diesen Fällen vorzugsweise solche, bei denen die Lähmung nach acuten fieberhaften Krankheiten (Typhus, Pocken) entstanden war. In anderen Fällen habe ich das Umgekehrte beobachtet; so bestand in einem Falle von Paraplegie in Folge von Sturz auf den Rücken exquisites Fussphänomen, aligemeiner Tremor des Beins bei gewissen Bewegungen desselben, dagegen keine Spur einer Contraction des Quadriceps; anstatt dessen fand jedesmal eine Gontraction in der Gegend des Tensor fasciae latae, yielleicht auch der Glutaeen statt. Constant fehlte das Unterschenkelphänomen, wie auch vom Fussphänomen angegeben, in allen untersuchten zweifellosen Fällen von Tabes dorsualis.
Westphal 1875. Über einige durch mechanische Einwirkung auf Sehnen und Muskeln hervorgebrachte Bewegungs‐Erscheinungen; p. 819-820
Occurrence of the lower leg phenomenon.
The minimal tapping on the patellar ligament resulting in extension of the lower leg caused by a sudden contraction of the quadriceps is found in a large number of cases in which the rhythmic foot movements can also be observed when the foot is dorsiflexed, and in hemiplegia (hemiparesis) as well as in paralyzed conditions of both lower extremities (paraplegia, paraparesis); in the former, the phenomenon, such as the foot phenomenon, is more pronounced on the paralyzed side, such that with the same strength of the stimulus (tapping) the contraction of the quadriceps is stronger on the more affected side, or a lesser stimulus is required to induce the contraction. The same is generally true of the paresis of both lower extremities.
However, there are not infrequently exceptions to this rule. In hemiplegia it happens that the lower leg phenomenon is equally strong on both sides but the foot phenomenon is only developed on the paralyzed side; also in individual cases, in the absence of the latter on the paralyzed foot, I have found the former to be present on the same paralyzed side…In paresis of both lower extremities, the lower leg phenomenon is sometimes very pronounced…Strangely (coincidentally?) among these cases there are mainly those in which the paralysis arose after acute febrile illnesses (typhus, smallpox). In other cases, I have observed the reverse; in one case of paraplegia, as a result of falling on the back, there was an exquisite foot phenomenon, general tremor of the leg during certain movements, but no trace of contraction of the quadriceps; instead, a contraction always took place in the region of the tensor fasciae latae, and perhaps also of the gluteal. The lower leg phenomenon was also constantly absent in all undoubted cases of tabes dorsualis examined.
Westphal 1875. Über einige durch mechanische Einwirkung auf Sehnen und Muskeln hervorgebrachte Bewegungs‐Erscheinungen; p. 819-820
Westphal-Variant Huntington’s Disease/Westphal-Strümpell Pseudosclerosis (1883)
Westphal-Variant Huntington’s Disease is a variant of Huntington’s disease characterized by a rigid and akinetic syndrome at the time of disease onset. Classically seen in juvenile-onset Huntington’s disease characterized by large CAG expansions, but may rarely be seen in patients with late-onset Huntington’s (>50-years old).
Westphal-Strümpell Pseudosclerosis refers to the neurological symptoms seen in Wilson’s disease; a genetic disorder characterized by excess copper storage in various body tissues. Wilson’s disease was initially known as Westphal-Strümpell pseudosclerosis for a number of years before Kinnier Wilson (1878-1937) published the pathoanatomical basis of the disease.
1883 – Westphal detailed the observations of two patients who had signs of gray matter degeneration but whose autopsies revealed no obvious disease. The observations spanned over a period of eleven years. Westphal noted facial rigidity and akinesia to be common symptoms between the two cases.
Due to the ambiguity of the disease etiology, two eponymous terms would spawn from Westphal’s case descriptions. To this day it is not known what the diseases Westphal actually are; it may be that, from the two cases he described, one was of pseudosclerosis and the other of Huntington’s disease.
German
English
Im Jahre 1872 beobachtete ich zuerst einen Krankheitsfall, der, obwohl der Symptomencomplex im Grossen und Ganzen sich dem vieler Fälle von multipler cerebrospinaler grauer Degeneration anzusehliessen schien, doch wegen einiger Besonderheiten mein Interesse in hohem Grade in Ansprueh nahm; die sehr viel spiiter erfolgte Autopsie ergab zur Ueberrasehung aller derer, welche den Kranken gekannt batten, einen wesentIich (makroskopiseh und mikroskopisch) negariven Befund. Später kam ein zweiter Fall in die klinische Behandlung, welcher, obwohl durch gewisse Erscheinungen besonders ausgezeichnet, dennoch eine Analogie zu dem erst beobachteten darzubieten schien, und bei dessen Autopsie auffälligerweise gleichfalls keine Veränderungen des Centralnervensystems, auch nicht durch die mikroskopische Untersuchung, aufgefunden werden konnten.
Analoge Erscheinungen bot die Gesichtsmuskulatur dar. Sehr eigenthümlich und nicht leicht zu schildern war zunächst der Gesichtsausdruck. Das Gesicht hatte bei beiden Kranken etwas Erstauntes und Stupides, verbunden mit etwas Starrem, Maskenartigem. Es war nicht der einfach stupide erstaunte Gesichtsausdruck eines paralytisch Geisteskranken, auch nicht der eines Idioten, ebenso wenig entsprach er der Physiognomik eines an Bulbärparalyse leidenden Kranken, sehon deshalb nicht, weil bei letzterem nur der untere Theil des Gesiehts schlaff und ausdruckslos zu sein pfiegt, vielmehr war das vorwiegende Moment eine gewisse Unbeweglichkeit und Starrheit tier Züge, die eine grössere Stupidität vortäuschte, als in der That vorhanden war, und deren Wirkung vermehrt wurde dutch das Ausbleiben des Lidschlages in der gewöhnlichen Häufigkeit und durch die mangelnde Beweglichkeit des Blickes…
Westphal 1883. Ueber eine dem Bilde der cerebrospinalen grauen Degeneration ähnliche Erkrankung des centralen Nervensystems ohne anatomischen Befund, nebst einigen Bemerkungen über paradoxe Contraction; p. 87, 122
In 1872 I first observed a case of illness which, although the symptom complex appeared to be largely the same as that of cerebrospinal gray-matter degeneration, nevertheless, because of some peculiarities, attracted my interest to a high degree. The autopsy, which was carried out much later, revealed an essentially (macroscopically and microscopically) negative finding to the surprise of all those who had known the patient. Later a second case came into the clinic, which, although particularly distinguished by certain phenomena, nevertheless seemed to offer an analogy to the first observed, and on the autopsy of which, strikingly, also had no changes in the central nervous system, not even by microscopic examination …
The facial muscles presented analogous phenomena. The facial expression was at first very peculiar and not easy to describe. There was something astonished and stupid about the face of both patients, combined with something rigid, mask-like. It was not the simply stupid, astonished facial expression of a paralytically insane patient, nor that of an idiot, nor did it correspond to the physiognomy of a patient suffering from bulbar paralysis, not because in the latter only the lower part of the face tends to be limp and expressionless, Rather, the predominant factor was a certain immobility and rigidity of the features, which simulated a greater stupidity than was actually present, and the effect of which was increased by the lack of blinking in the usual frequency and by the lack of mobility of the gaze…
Westphal 1883. Ueber eine dem Bilde der cerebrospinalen grauen Degeneration ähnliche Erkrankung des centralen Nervensystems ohne anatomischen Befund, nebst einigen Bemerkungen über paradoxe Contraction; p. 87, 122
In terms of Huntington’s disease, Joseph Peretti would be the next to describe Westphal’s variant in 1885 and would be the first to accurately give the diagnosis of Huntington’s disease.
In terms of pseudosclerosis, Adolf von Strümpell would, in 1897, present a larger study discussing the findings of Westphal and other authors, alongside cases seen himself.
Westphal syndrome (1885)
A familial form of intermittent hypocalcaemic paralysis characterized by periodic attacks of flaccid paralysis and areflexia which can be precipitated by infusions of glucose and insulin, eating a large meal, or administration of adrenaline. Age of onset is usually between 7-21 years.
The syndrome was first described by William Musgrave (1655–1721) in the 1700s.
1885 – Westphal first described a case of the syndrome in a 12-year old boy who was referred to him from Friedrich von Frerichs’ clinic, who suffered attacks of temporary paralysis with the electrical excitability of the muscles being completely extinguished.
German
English
Der jugendliche Patient war am 7. Januar 1885 auf die Klinik aufgenommen worden wegen eines Anfalles von Lähmung aller vier Extremitäten; es ist nicht notirt, wie lange derselbe dauerte…Am 30. Abends Beginn eines neuen Anfalles von Lähmung, die am 31. bis auf geringe Bewegungen mit der Hand vollständig ist…wurde Patient der Nervenklinik übergeben; der Anfall begann schon nachzulassen, indess waren die willkürlichen Bewegungen noch aufgehobeu mit Ausnahme geringer Finger- and Fuss- bewegongen; die Glieder fielen, emporgehoben, schlaff herab, nur einmal schien es, als wenn Patient das passiv emporg hobene Bein vorübergehend in der Stellung zn halten im Stande war. Wurde er aus dem Bett genommen, so sank er sofort in die Kniee. Bereits nach einigen Stunden schwanden die Läh¬ mungserscheinungen nach und nach; eine genauere Untersuchung wurde bei diesem Anfall nicht vorgenommen…
Die Untersuchung des Knaben während der Zeit ausserhalb der Anfälle ergab absolut keinerlei Störungen weder im Bereiche des Nervensystems noch anderer Organe (namentlich auch keine Milzvergrösserung). Der Knabe war für sein Alter kräftig entwickelt, in der Gesichtsbildung fiel höchstens eine gewisse Schmalheit der Lidspalten auf. Die Wangen zeigten eine gesunde Röthung…
Electrische Erregbarkeit. Mit den stärksten faradischen Strömen sind von den Nervenstämmen der oberen und unteren Extremitäten nur sehr schwache Zuckungen zu erzielen, während Patient bei der Stärke des Stromes vor Schmerz aufschreit, und der Vergleich an einem Gesunden lehrt, dass der Strom sehr kräftig ist.
Westphal 1885. Über einen merkwürdigen Fall von periodischer Lähmung aller vier Extremitäten mit gleichzeitigem Erlöschen der elektrischen Erregbarkeit während der Lähmung; p 489-490.
The adolescent patient had been admitted to the clinic on January 7, 1885, because of an attack of paralysis in all four extremities; it is not noted how long it lasted … On the evening of the 30th a new attack of paralysis began, which on the 31st was complete except for slight movements of the hand … the patient was transferred to the mental hospital; the attack was already beginning to subside, but no voluntary movements were able to be performed with the exception of slight movements of the fingers and feet; the limbs fell limply when lifted, and only once did it appear as if the patient was temporarily able to hold up the passively lifted leg. If he was taken out of bed, he would immediately drop to his knees. After a few hours, the symptoms of paralysis gradually disappeared; no closer examination was made of this attack…
Examination of the boy during the time outside of the attacks revealed absolutely no disturbances, neither in the area of the nervous system nor in other organs (notably no enlargement of the spleen). The boy was well developed for his age, the most striking thing in his facial features was a certain narrowing of the eyelids. The cheeks showed a healthy flush…
Electric excitability. With the strongest faradic currents, the nerve trunks of the upper and lower extremities produced only very slight twitches, while the patient cried out in pain at the strength of the current, and comparison with a healthy person showed that the current was very strong.
Westphal 1885. Über einen merkwürdigen Fall von periodischer Lähmung aller vier Extremitäten mit gleichzeitigem Erlöschen der elektrischen Erregbarkeit während der Lähmung; p 489-490.
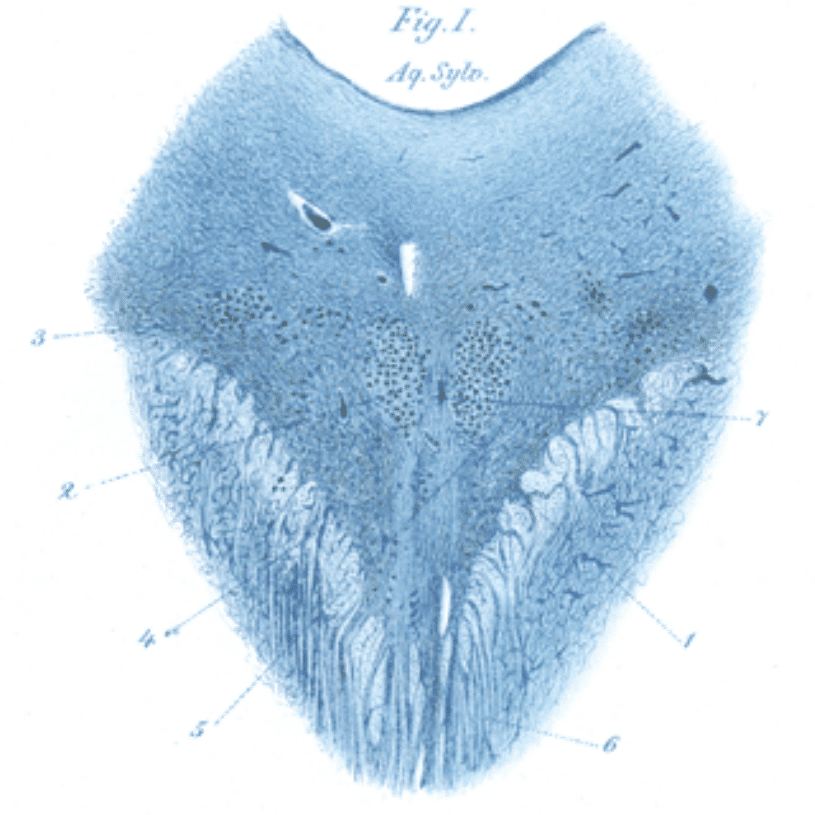
Edinger-Westphal nucleus (1887)
Eponymously used to describe two different, albeit somewhat intermingled, cell groups found in the midbrain. More commonly refers to a pair of pre-ganglionic nuclei involved in the parasympathetic innervation of the iris sphincter muscles and ciliary muscles eyes, responsible for pupillary constriction and lens accommodation. However, may also refer to a group of centrally projecting neurons involved in sympathetic, consumptive and stress-related functions.
1885 – First described by Ludwig Edinger where he demonstrated the existence of the nucleus in a fetus.
1887 – Westphal proved the existence of the nucleus in adults, where he described the autopsy of a 44-year old man with progressive external ophthalmoplegia who still retained pupillary constriction and lens accommodation. From this case, Westphal was able to infer that it was a small-celled neuronal group above the oculomotor nuclei which was responsible for the innervation of these functions.
German
English
Wir können aber hier offenbar nur den grösseren bekannten Oculomotoriuskern für die Degeneration in Anspruch nehmen, da die medialen und lateralen Kerne keine Spur von Atrophie zeigen… Es scheint daraus gefolgert werden zu müssen, dass alle äusseren Augenmuskeln von dem ursprünglich allein bekannten Oculomotoriuskern jedenfalls zum grössten Theile innervirt werden, wenngleich der Beweis, den unser Fall dafür liefert, mehr ein negativer ist.
Welchem Zwecke könnten nun aber die gesund gebliebene mediale und laterale Gruppe dienen? Eine Antwort darauf liegt sehr nahe; es könnten möglicherweise die innneren glatten Augenmuskeln, die Verengerer der Pupillen und die Accommodationsmuskeln, von diesen Gruppen aus innervirt warden.
Westphal 1887. Ueber einen Fall von chronischer progressiver Lähmung der Augenmuskeln (Ophthalmoplegia externa) nebst Beschreibung von Ganglienzellengruppen im Bereiche des Oculomotoriuskerns; p. 867
We can assume that only the oculomotor nucleus has degenerated, as the medial and lateral nuclei show no trace of atrophy…it was previously concluded that all external eye muscles are innervated by the main oculomotor nuclei, although the evidence provided by our case goes against this notion.
So, what purpose could the healthy medial and lateral group serve? The answer is obvious; the internal smooth muscles of the eye, the constrictor of the pupils and the accommodation muscles, could possibly be innervated from these groups.
Westphal 1887. Ueber einen Fall von chronischer progressiver Lähmung der Augenmuskeln (Ophthalmoplegia externa) nebst Beschreibung von Ganglienzellengruppen im Bereiche des Oculomotoriuskerns; p. 867
Key Medical Attributions
Modern Homosexuality (1870)
The French philosopher Michel Foucault (1926-1984) credits Westphal for the birth of modern homosexuality. In 1870, Westphal published a paper on ‘contrary sexual feelings’, where he described in great detail a case of a 20-year old man and a 35-year old woman who were dealing with “an innate perversion of sexual feelings”, later identified to be homosexuality. Although deeming the behavior to be potentially pathological, Westphal was also aware that not all such behavior was pathological in nature.
German
English
Schliesslich will ich, um allen Missdeutungen von vorn herein vorzubeugen, ausdrücklich erklären, dass es mir nicht in den Sinn kommt, alle Individuen, welche sich widernatürlicher Unzucht hingeben, für pathologische Naturen zu erklären! Ich weiss sehr wohl, dass dies nicht der Fall ist. Aber wie es pathologischen Diebstahl und Mord gibt, so auch eine pathologische Geschlechtsverirrung, ohne dass darum die grosse Mehrzahl der Fälle von Diebstahl, Mord und widernatürlicher Unzucht pathologisch wäre.
Westphal 1870. Die conträre Sexualempfindung, Symptom eines neuropathischen (psychopathischen) Zustandes; p. 108
Finally, in order to prevent all misinterpretations from the outset, I want to state that it does not occur to me to declare all individuals who indulge in unnatural fornication to have pathological natures! I know very well that this is not the case. But just as there is pathological theft and murder, there exists also a pathological sexual aberration, albeit the majority of cases of theft, murder and unnatural fornication are not pathological.
Westphal 1870. Die conträre Sexualempfindung, Symptom eines neuropathischen (psychopathischen) Zustandes; p. 108
Agoraphobia (1872)
Westphal was the first to coin the term ‘agoraphoria’, doing so in his 1872 publication, Die Agoraphobie, eine neuropathische Erscheinung. He described observing three of his male patients exhibiting extreme anxiety and feelings of dread when they had to enter certain public areas of the city.
German
English
Diese Furcht vor dem Durchschreiten von Plätzen resp. Strassen stellte derart das Hauptphänomen dar, dass ich, obwohl sie sich noch auf gewisse andere Situationen bezog, und daher die gewählte Bezeichnung — denn eine solche schien mir wünschenswerth — nicht ganz erschöpfend ist, das Wort Agoraphobie, Platzfurcht, dafür bilden zu können meinte.
Westphal 1872. Die Agoraphobie, eine neuropathische Erscheinung; p. 138
This fear of passing through squares or streets was so much the main phenomenon that, although it referred to certain other situations, and therefore the name chosen — because such a name seemed desirable to me — is not quite exhaustive, I thought I could use the word agoraphobia to describe it.
Westphal 1872. Die Agoraphobie, eine neuropathische Erscheinung; p. 138
Narcolepsy and Cataplexy (1877)
Westphal was also the first physician to provide a clinical description of narcolepsy and cataplexy in his 1877 paper, Eigentümliche mit Einschlafen verbundene Anfälle, where he details two cases he presented at the Berlin Medical and Psychological Society meeting in July of 1876. Westphal emphasized that the attacks involved loss of muscle tone without any associated loss of consciousness, and that there was “persistent night-time sleeplessness” in his patients; features commonly seen in cataplexy and narcolepsy respectively. Alongside his description of the cases, Westphal was also the first to describe the possible existence of familial cataplexy, noting that the mother of his 36-year old male patient also suffered from longstanding, recurrent episodes of cataplexy albeit of milder severity. However, Westphal could not discern the cause of the attacks and it was Jean-Baptiste-Édouard Gélineau (1828-1906) who coined the term narcolepsie in 1880.
Controversies
Not to be confused with his son, Alexander Karl Otto Westphal (1863–1941), who was also a psychiatrist and is associated with the Westphal-Piltz syndrome (neurotonic pupillary reaction).
Major Publications
- Westphal, C. Die conträre Sexualempfindung, Symptom eines neuropathischen (psychopathischen) Zustandes. Archiv für Psychiatrie und Nervenkrankheiten. 1872;2:73–108 [modern homosexuality]
- Westphal C. Die Agoraphobie, eine neuropathische Erscheinung. Archiv für Psychiatrie und Nervenkrankheiten. 1872;3:138-161. [agoraphobia]
- Westphal C. Ueber eine Affection des Nervensystems nach Pocken and Typhus. Archiv für Psychiatrie und Nervenkrankheiten. 1872;3:376–406. [Leyden-Westphal ataxia]
- Westphal C. Über einige Bewegungs-Erscheinungen an gelähmten Gliedern: II Über einige durch mechanische Einwirkung auf Sehnen und Muskeln hervorgebrachte Bewegungs‐Erscheinungen. Archiv für Psychiatrie und Nervenkrankheiten 1875;5:803–834 [Erb–Westphal symptom]
- Westphal C. Eigentümliche mit Einschlafen verbundene Anfälle. Archiv für Psychiatrie und Nervenkrankheiten. 1877;7:631–635. [narcolepsy and cataplexy]
- Westphal C. Ueber eine dem Bilde der cerebrospinalen granen Degeneration ähnliche Erkrankung des centralen Nervensystems ohne anatomischen Befund, nebst einigen Bemerkungen über paradox Contraction. Archiv für Psychiatrie und Nervenkrankheiten 1883;14:87-134 [Westphal-variant Huntington’s disease/Westphal-Strümpell pseudosclerosis]
- Westphal C. Über einen merkwürdigen Fall von periodischer Lähmung aller vier Extremitäten mit gleichzeitigem Erlöschen der elektrischen Erregbarkeit während der Lähmung. Berliner Klinische Wochenschrift 1885,22:489–491, 509–511. [Westphal syndrome]
- Westphal C. Ueber einen Fall von chronischer progressiver Lähmung der Augenmuskeln (Ophthalmoplegia externa) nebst Beschreibung von Ganglienzellengruppen im Bereiche des Oculomotoriuskerns. Archiv für Psychiatrie und Nervenkrankheiten 1887;18:846-871 [Edinger–Westphal nucleus]
References
Biography
- Nekrolog. Carl Friedrich Otto Westphal (1833 – 1890). Archiv für Psychiatrie und Nervenkrankheiten 1890;21:I-XXII
- Professor Karl Westphal. Br Med J. 1890;1(1519):332.
- Bibliography. Westphal, Carl Friederich Otto. WorldCat Identities
Eponymous terms
- Edinger L. Über den Verlauf der centralen Hirnnervenbahnen mit Demonstrationen von Präparaten. Arch Psychiatr Nervenkrankheiten. 1885;16:858–859.
- Tyler KL, McHenry LC Jr. Fragments of neurological history. The knee jerk and other tendon reflexes. Neurology. 1983 May;33(5):609-10.
- Lanska DJ. [History of the reflex hammer] Tidsskr Nor Laegeforen. 1998;10;118(30): 4666-8
- Schenck CH, Bassetti CL, Arnulf I, Mignot E. English translations of the first clinical reports on narcolepsy and cataplexy by Westphal and Gélineau in the late 19th century, with commentary. J Clin Sleep Med. 2007;3(3):301-311.
- Kozicz T et al. The Edinger-Westphal nucleus: a historical, structural, and functional perspective on a dichotomous terminology. J Comp Neurol. 2011 Jun 1;519(8):1413-34.
- Ciammola A, Sassone J, Poletti B, Mencacci N, Benti R, Silani V. Atypical Parkinsonism Revealing a Late Onset, Rigid and Akinetic Form of Huntington’s Disease. Case Rep Neurol Med. 2011;2011:696953.
Eponym
the person behind the name
Lewis is an RMO at Royal Perth Hospital. He is currently interested in critical care medicine.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
