
![]()
Common Krait
The Common Krait is one of the “Big Four” venomous snakes of India. The snakes known for causing most medically significant bites on the Indian subcontinent. The snake being nocturnal, most bites occur during the night. The snake is distributed all across India, Pakistan, and Srilanka.
The classic presentation of envenoming will be a patient presenting in the morning without any history of bite or fang marks with abdominal pain or discomfort, followed by a symmetrical descending paralysis.
Resus
- Potential to be immediately life-threatening, the patient should initially be managed in an area capable of resuscitation.
- Early threats to life include signs of descending flaccid paralysis.
- If respiratory failure occurs regardless of whether antivenom has been given, provisions should be made to secure the airway and ventilate the patient.
Risk Assessment
Typical symptoms include:
- No pain at the bite site – puncture wounds may not be apparent
- No ecchymosis, swelling, or any other local sign. At times, the bite described as mosquito bite
- Non-specific symptoms include numbness, paresthesias, aching of extremities, headache and abdominal pain.
- It is vital to recognize the patients of Krait bites early before the onset of significant neurotoxicity when the antivenom is more effective
- Neurotoxicity is slow in onset (usually within 2 hours) and progresses over time. The early features include ptosis, blurred vision, diplopia and difficulty swallowing.
Supportive Care
- Symptomatic relief – antiemetics, analgesia.
- Intubation and Ventilation if respiratory failure is present.
- Pressure bandage with Immobilisation (PBI) – Should have been applied pre-hospital, if not apply while awaiting initial investigations.
PBI Video
Investigations
1. Laboratory Tests (At presentation, 1 hour post PBI removal, 6 and 12 hours following the bite): FBC, EUC, CK, INR, APTT, Fibrinogen, D-dimer, Forced expiratory flow, Arterial oxygen saturation. If there is no evidence of envenoming at 24 hours after the bite, the patient is fit for discharge (although not during the night as subtle neurotoxicity maybe missed).
2. Krait envenoming is characterised by descending Paralysis
4. Clinical exam for descending paralysis and spirometry can be a good measure of pending respiratory decline alerting you to the potential for intubation and ventilation.
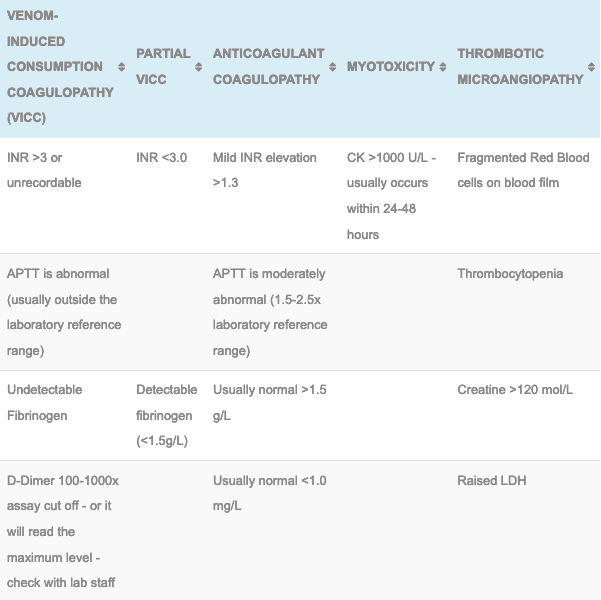
Laboratory Results seen in the Asian Snake Envenomations
Differential Diagnosis:
- Krait and Cobra snake envenomations are very similar, the main difference between the two is significant local symptoms in case of Cobra.
- Coral snakes are also similar to the Krait causing minimal local symptoms and descending paralysis.
Antivenom
- Polyvalent Snake Antivenom: Active against the “Big Four” (Common Cobra, Common Krait, Russell’s Viper and Saw scaled Viper) used in the treatment of envenomation by the Krait.
- It will not reverse paralysis but dose halt further progression.
Disposition
- All patients must be observed in a hospital capable of managing a potential snake bite envenomation, this involves adequate laboratory cover and the ability to administer antivenom and manage potential anaphylaxis.
- Patients with no clinical evidence of paralysis or coagulopathy at 24 hours post bite are not envenomed and maybe discharged in daylight hours.
- Envenomed patients can be discharged following antivenom. If paralysis has occurred the resulting disability will determine if discharge is feasible.
References and Additional Resources:
Additional Resources:
- Approach to the Snakebite Patient
- Tox Conundrum 005 – Snakebite vs Stickbite
- Tox Conundrum 026 – Snakebite Envenoming Challenge
References
- Bradley D. Riley, Anthony F Pizon, Anne Michelle Ruha. Snakes and other Reptiles. Goldfrank’s Toxicologic Emergencies 2011: 1601-1610
- Aniruddh Ghose, Julian White. Asian Snakes. Critical Care Toxicology 2017: 2343- 2403
- Standard treatment guidelines. Management of snakebite 2016. Ministry of Health and Family welfare, Government of India

Toxicology Library
TOXINS

Dr Shiuli, MBBS, MD. Currently serving as Associate Professor in Forensic Medicine & Toxicology at King George's Medical University, Lucknow (India).