
![]()
CT Case 046
A 60-year-old man presents with severe shortness of breath on a background of ischaemic cardiomyopathy, episodes of acute pulmonary oedema and a 50-pack year smoking history.
The end-of-the-bed-o-gram looks like another episode of acute pulmonary oedema. He is sat in a tripod position, tachypnoeic to mid 30s, sats 82% on RA, HR 130, SBP 160, and afebrile.
Auscultation of his chest however, contradicts this diagnosis with the left lung field demonstrating normal breath sounds and near absent breath sounds in the right lung field
With the long smoking history, perhaps it could be a pneumothorax secondary to underlying emphysematous lung disease?
A CXR was performed

Describe and interpret the CXR
CXR INTERPRETATION
No, it’s not a pneumothorax.
The right hemi-thorax is slightly under expanded compared to the left. However, there are lung markings all the way to the peripheries.
There are also no features of acute pulmonary oedema.
There is however, a right hilar mass.
If you look VERY closely, you will also see a small peripheral nodule in the midzone of the right lung.

The astute registrar caring for this patient, has a suspicion this could be a bronchial obstruction, and given the smoking exposure, likely secondary to a new diagnosis of lung cancer.
He went on to have a CT scan of the chest
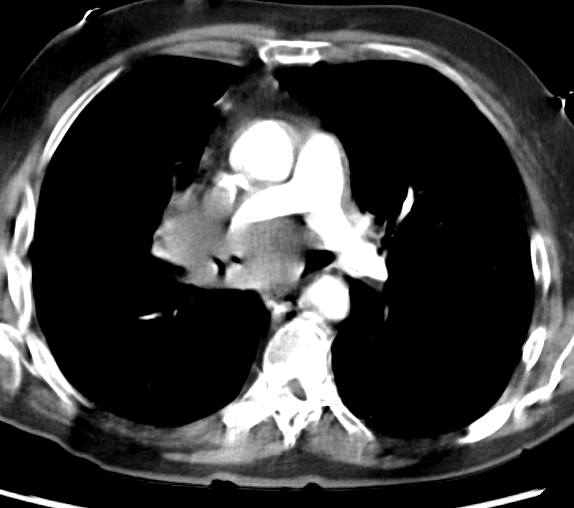

CT INTERPRETATION
The case shows a central soft tissue density in the right hilar region with invasion of mediastinal structures (the carina, the right pulmonary artery and SVC).
On the CT scan, we can see the subpleural nodule in the right upper lobe more clearly.
This is in keeping with presence of a primary lung cancer and associated mediastinal lymphadenopathy.
Sometimes, as in this case, the lymphadenopathy appears larger than the primary lung lesion. Typically, lung cancers cause cut-off of bronchi resulting in distal atelectasis.
CT imaging can aid if differentiating the type of lung cancer. Of the Non-small cell lung carcinomas, which comprise almost 80% of cases of lung cancers;
- Adenocarcinoma tends to be more peripheral
- Squamous cell carcinoma when central tends to cavitate
- Bronchioalveolar carcinoma has a more confusing radiological appearance demonstrating lung consolidation similar to pneumonia. Therefore, presence of a non-resolving pneumonia should raise suspicion for the same


CLINICAL CORRELATION
Unfortunately, our registrar was right. The CT findings were highly suspicious for new diagnosis of lung cancer. A diagnosis was confirmed on bronchial biopsy.
This patient’s acute respiratory distress responded well to a period of NIV. The positive pressure ventilation alleviated some of this work of breathing, and helped to splint open his right bronchi and re-expand the right lung.
He has since commenced inpatient chemotherapy.
Bonus images:
As part of his work-up this patient underwent a PET-CT.
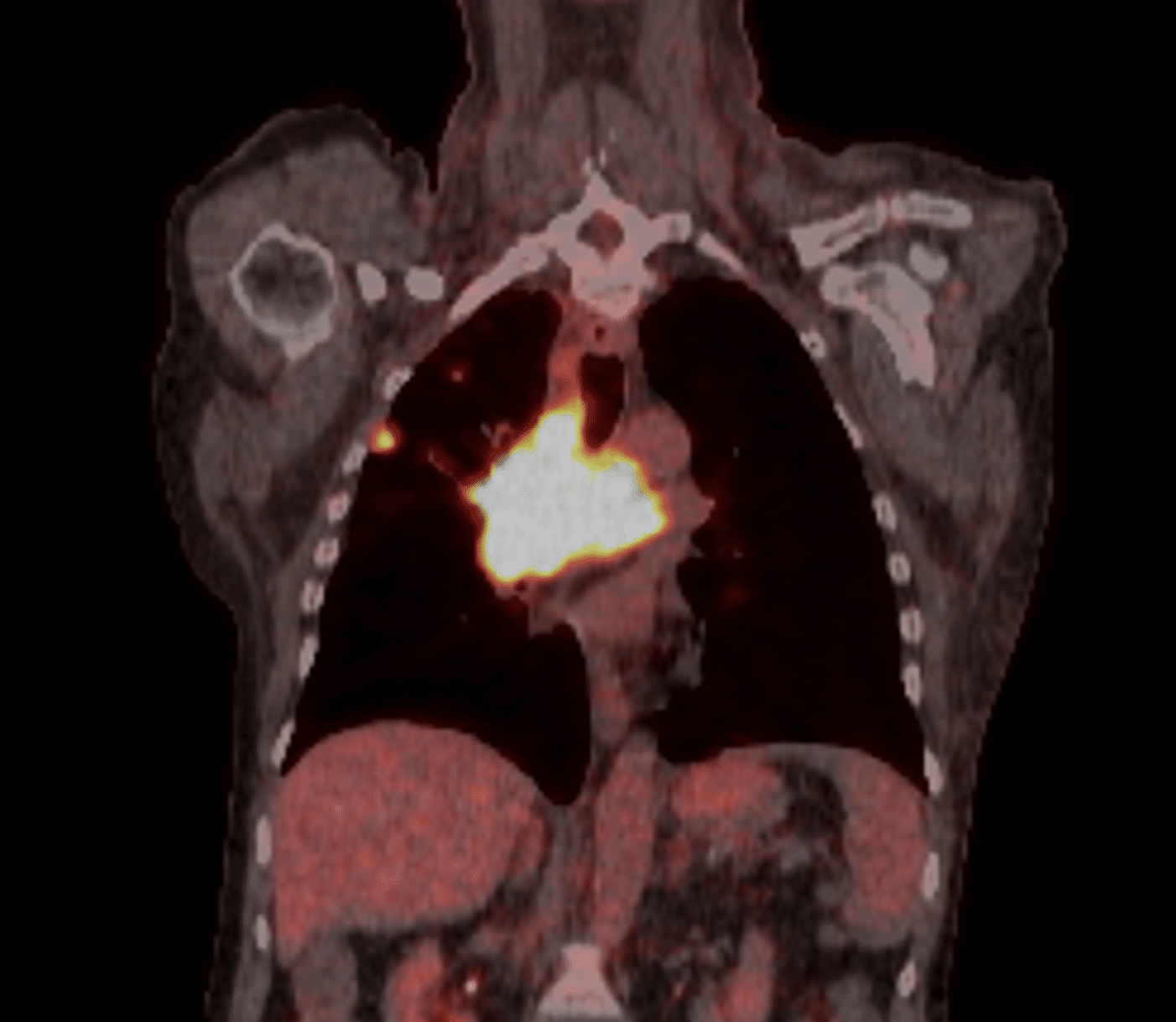
PET scan interpretation
We see the subpleural nodule shows FDG avidity.
PET-CT is a type of dual-modality imaging, it combines the advantages of both PET and CT.
In a PET (positron emission tomography) scan, a radiolabelled compound, often FDG (F-18 fluorodeoxyglucose) is injected intravenously. Tumour cells, due to their high metabolic rate, have an increased uptake of FDG. The metabolite of FDG accumulates in these cells and its presence is then quantified in a PET scan.
The simultaneously acquired CT scan provides superior anatomical detail and spatial resolution compared to the PET scan. The PET and CT scans are performed sequentially with the patient in the same position. Images can then be fused together as we see here.

References
- Panunzio A, Sartori P. Lung Cancer and Radiological Imaging. Curr Radiopharm. 2020;13(3):238-242.
- Fahrenhorst-Jones T. PET-CT (overview). Radiopaedia
TOP 100 CT SERIES

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).

Provisional fellow in emergency radiology, Liverpool hospital, Sydney. Other areas of interest include paediatric and cardiac imaging.

Emergency Medicine Education Fellow at Liverpool Hospital NSW. MBBS (Hons) Monash University. Interests in indigenous health and medical education. When not in the emergency department, can most likely be found running up some mountain training for the next ultramarathon.
