
![]()
CT Case 045
A 95-year-old female is transferred from a nursing home complaining of severe generalised abdominal pain and fevers. Her only past medical history is atrial fibrillation
On examination she very unwell and abdominal examination revealed diffusely peritonitic.
Vital signs: HR 120 (irregular), SBP 80/50, RR 28, 92% RA, temp 37.9.
Initial investigations show a lactate of 8, and WCC of 24
A CT abdomen was performed
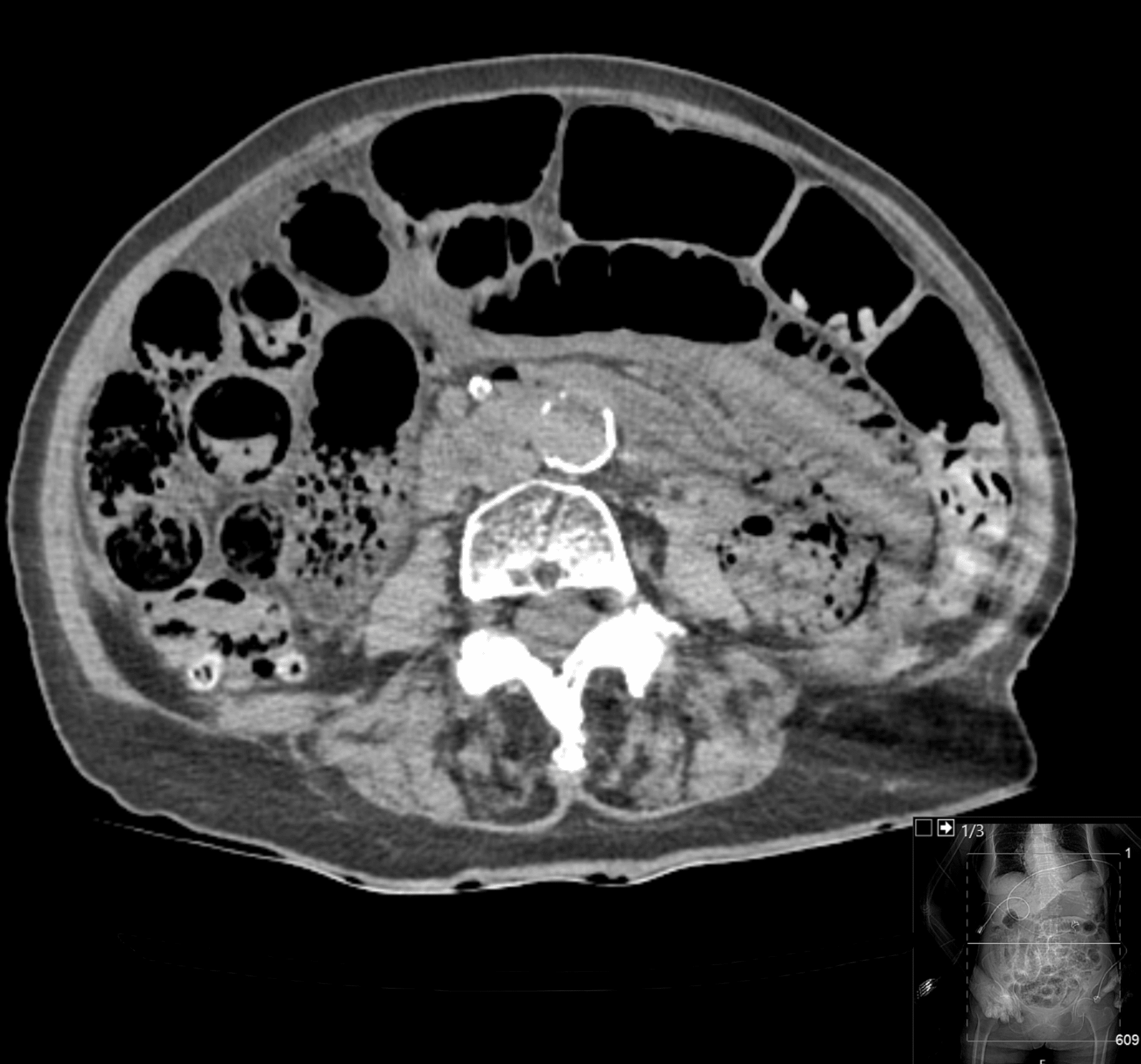

Describe and interpret the CT scan
CT INTERPRETATION
There is extensive intramural air in the small bowel wall. The small bowel is also distended, however no localised transition point is seen.
Widespread bowel ischaemia is the likely cause of these findings.
There is also extensive intrahepatic gas. The gas reaches the peripheries of the liver, this distribution is consistent with portal venous gas.
This CT scan demonstrates extensive pneumatosis intestinalis, that is the presence of intramural air within the bowel wall. Though occasional this can appear as a normal finding in asymptomatic patients, it usually represents critical findings such as ischemia, infection or toxic injury.
Portal vein gas is seen as a consequence of the splanchnic circulation draining into the portal vein.


With the retrospectoscope…is the chest X-ray helpful?

CT INTERPRETATION
This would be very easily overlooked!
However, with the advantage of knowing what we’re looking for, we can see there is a radiolucent area overlying the liver shadow, reaching the peripheries of the liver. This again represents the portal venous gas. We can even just make out the branching pattern of the gas.

CLINICAL CORRELATION
This is a case of extensive mesenteric ischaemia which has resulted in pneumatosis intestinalis and subsequently portal venous gas.
There are two patterns of intrahepatic branching gas.
- Portal venous gas, as we see here
- Portal venous gas reaches the Peripheries
- Pneumobilia (gas within the common bile duct and biliary system)
- Common bile duct gas is Central
Typically, we think of portal venous gas being secondary to a more sinister cause, and pneumobilia being due to a more benign cause. Although as you’ll see from the list below, even some of the causes of pneumobilia can be concerning
| Portal Venous Gas | Pneumobilia |
| Ischaemic bowel Intraabdominal sepsis; diverticulitis, infectious colitis, haemorrhagic pancreatitis Necrotizing enterocolitis Necrotic/ulcerated colorectal cancer Inflammatory bowel disease Perforated peptic ulcer Bowel obstruction | Biliary tree infection; cholangitis, emphysematous cholecystitis Liver abscess Following instrumentation; ERCP Incompetent sphincter of Oddi Biliary-enteric fistula |
The extent of bowel ischaemia in this patient and the severity of the disease were deemed non-recoverable, and this patient was managed with comfort measures.
References
- Hartung MP. Abdominal CT: closed loop. LITFL
TOP 100 CT SERIES

Emergency Medicine Education Fellow at Liverpool Hospital NSW. MBBS (Hons) Monash University. Interests in indigenous health and medical education. When not in the emergency department, can most likely be found running up some mountain training for the next ultramarathon.

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).

Provisional fellow in emergency radiology, Liverpool hospital, Sydney. Other areas of interest include paediatric and cardiac imaging.