
![]()
CT Case 104
A 45 year old female presents with shoulder pain following a seizure.
She is found to have a swollen painful left shoulder with reduced range of motion in all directions. Her left arm is neurovascularly intact.
An X-ray of the shoulder found an enlocated shoulder with an irregularity around the glenoid rim.
A CT of the left shoulder is arranged.


Clinical Pearls
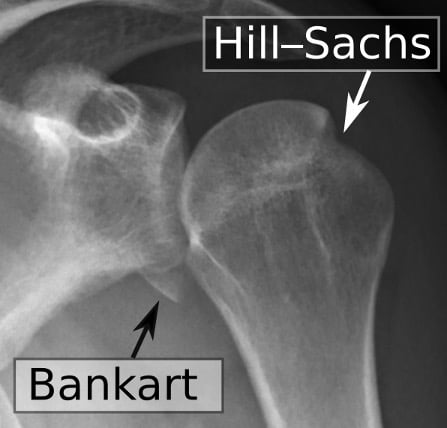
Shoulder dislocations may be complicated by Hill-Sachs or Bankart lesions. These often occur during shoulder dislocations when the humeral head is forcibly impacted on the glenoid rim. These injuries can contribute to future shoulder instability, and their management is determined by the size of the injury and associated instability of the shoulder joint.
Hill-Sachs defects are cortical depressions of the posterolateral aspect of the humeral head. They occur in up to 40% of anterior shoulder joint dislocations (1) and are best seen on AP X-rays with the arm held in internal rotation. These injuries may be managed nonoperatively if the bony defect is small (<20% of the articular surface of the humeral head) and the glenohumeral joint remains stable during desired activities (3). Surgical management involves bone grafting or placement of soft tissue within the defect.(3).
Bankart lesions are injuries at the anteroinferor aspect of the glenoid labrum complex. They are classified as bony Bankart lesions (bone fragment avulsed) and soft tissue Bankart lesions (no bone avulsed). Management of bony Bankart lesions is similar to that of Hill-Sachs deformities in that these injuries are managed nonoperatively if the bony defect is <20% of the surface area of the inferior glenoid (5). Soft Bankart lesions occurring in young patients with first-time dislocation are often managed with arthroscopic repair. Surgical management involves suturing the labral fragment back to the glenoid rim using suture anchors. Early discussion with Orthopaedic specialists is recommended to guide management.
This patient was placed in a broad arm sling and referred to orthopaedics outpatient rooms for review in 2 weeks from time of injury.
Describe and interpret the CT scan
1. Hill-Sachs deformity in the posterior aspect of the humerus.


2. Comminuted displaced osseous (bony) Bankart lesion involving the anterio-inferior glenoid fossa (6-10 o’clock).


3. Comminuted laterally displaced fracture of the coracoid process.
4. Associated joint effusion and surrounding soft tissue haematoma.
References
- Riebel GD, McCabe JB. Anterior shoulder dislocation: a review of reduction techniques. Am J Emerg Med. 1991 Mar;9(2):180-8.
- Cadogan M. Hill-Sachs defect. Eponymictionary
- Provencher MT, Frank RM, Leclere LE, Metzger PD, Ryu JJ, Bernhardson A, Romeo AA. The Hill-Sachs lesion: diagnosis, classification, and management. J Am Acad Orthop Surg. 2012 Apr;20(4):242-52.
- Cadogan M. Bankart Lesion. Eponymictionary
- Bankart ASB. Recurrent or habitual dislocation of the shoulder joint. Br Med J. 1923 Dec 15; 2(3285): 1132–1133.
TOP 100 CT SERIES

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney

FACEM, MBBS (Hon), B. Pharm. Emergency Medicine Education Fellow at Liverpool Hospital, Australia. Special interests in clinical education, ECG interpretation and diagnostic ultrasound. Proud father and husband, sadly a golf tragic

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).