
![]()
Hill-Sachs defect
Hill-Sachs defect: Cortical depression of posterolateral head of the humerus related to impaction of the humeral head with inferior glenoid in anterior shoulder dislocation. Often associated with a Bankart lesion of the glenoid.
The resultant lesion predisposes the shoulder joint to recurrent dislocations, the lesion is larger in relation to the number of dislocations

Prior to the 1940 publication of Harold Arthur Hill (1901-1973) and Maurice David Sachs (1909-1987), this type of defect was already known as a sign of dislocation, but its mechanism and evolution were unknown. Between 1832 and 1930, there were many case reports which described the pathologico-anatomic findings in humeral heads resected for the relief of chronic or habitual dislocation. In all these cases there was such a similarity in the change found by the various operators that the groove or excavation became known as the ‘typical defect.’ A composite description of these resected specimens may be summed up as follows:
The defect is located posterior and medial to the greater tuberosity on the posterolateral aspect of the articulating surface of the humeral head. The groove is navicular or wedge-shaped and its average measurements are 2.5 cm. in length (cephalocaudad), 1.5 cm. in width, and 0.75 cm. in depth. The defect is demarcated from the surrounding normal bone by sharp or vertically projecting walls, which in the larger defects stand at a right-angle to each other
Hall, Sachs 1940: 690
Hill and Sachs provided evidence that the particular X-ray views were important in revealing the defect
Compression fractures of the humeral head, unless quite large, will frequently be overlook ed unless the x-ray studies are made with the possibility of such in mind. A stereoscopic anteroposterior examination with the arm adducted and in external rotation is not adequate to demonstrate the defect in many instances. An anteroposterior projection made with the arm in marked internal rotation is essential…With marked internal rotation, the posterolateral aspect of the head is viewed in profile so that the length and depth of the compressed area may be evaluated
Hall, Sachs 1940: 694

(Left) Diagram of an x-ray of a normal humerus in internal rotation.
(Right) Diagram of an x-ray of a humerus in internal rotation, showing defect.
Hall, Sachs 1940: 691
CT imaging (CT Case 104)


History of the Hill-Sachs defect
1832 – Malgaigne noted that following anterior shoulder dislocation a bony defect in the humeral head could be present
Original
English
“Amenée donc à l’Hôtel-Dieu près d’un mois après l’accident, ce qui frappa d’abord, ce furent les symptômes suivans: saillie de l’acromion, aplatissement du deltoïde, le coude écarté du tronc et n’en pouvant être rapproché, le bras ne pouvant s’élever vers la tête; enfin dans l’aisselle, une saillie évidemment osseuse. C’étaient bien là les signes de la luxation; mais ces mêmes signes accompagnent aussi la fracture”
“Admitted to the Hotel-Dieu nearly a month after the accident, what was most evident, were the following symptoms: protrusion of the acromion, flattening of the deltoid, the elbow separated from the trunk, unable to be approximated, the arm unable to be lifted to the head; finally, in the axilla, an evidently bony protrusion. These were indeed the signs of the luxation; but these same signs accompany also the fracture”
1861 – Sir William Henry Flower (1831-1899) reported upon 41 shoulder specimens collected from all the pathologic museums of London. He described cases which showed rupture of the tendons inserted upon the greater tuberosity, fracture of the tuberosity, or the presence of a groove excavated on the articular head posterior to the greater tuberosity. [Transactions, 1861]
1880 – Sir Frederik S. Eve (1853-1916) reported on a case confirming that such defects do occur immediately following a single injury to a shoulder previously proven to be normal.
Thomas B – 36, was knocked down by a train while at work on the line. He was admitted to St. Bartholomew’s Hospital with a a sub-coracoid dislocation of the right humerus. The dislocation was extremely easily reduced by traction on the limb with the heel in the axilla. The patient died twelve hours after the accident from injuries to the thorax.
On opening the joint a deep indentation is seen on the posterior surface of the head, produced by forcible impaction on the margin of the glenoid cavity. The formation of the groove partially accounts for the slight damage to the capsule, as the head of the bone, having lodged on the margin of the glenoid cavity, was thus prevented from passing further inwards on the surface of the scapula. The groove was situated at the extreme margin of the articular surface, showing that the head was entirely separated from the glenoid cavity
Eve, 1880
1906 – Georg Clemens Perthes (1869 – 1927) recognised that the inferior glenoid fracture with detachment of the labrum caused instability of the shoulder and emphasized reattachment of the labrum to stabilize the joint
Original
English
Die operative Behandlung der rezidivierenden Schultergelenksluxation ist noch kein abgeschlossenes Kapitel der Chirurgie…Bedeutungsvoller scheint mir vielmehr in einer gewissen Gruppe von Fällen der Abriß der am Tuberculum majus inserierenden Muskeln, und in einer anderen der Abriß des Labrum glenoidale am inneren Pfannenrande. Die Rücksicht auf diese pathologischen Veränderungen führte mich dazu, in zwei Fällen die verloren gegangene Insertion der Muskeln am Tuberculum majus wiederherzustellen, in einem weiteren Fall die am inneren Pfannenrand abgesprengte Gelenklippe wieder zu befestigen, während in einem vierten Falle nur die Verkleinerung und Verstärkung der erweiterten und erschlafften Kapsel ausgeführt wurde.
The operative treatment of recurrent shoulder subluxations is still no concluded chapter in surgery…Of greater significance it would seem to me, is in a certain group of cases the tearing of the muscles inserting on the major tubercle, and in another group, the tearing of the glenoid labrum on the inner glenoid fossa. The consideration of these pathological changes led me to reconstruct the lost insertion point of the muscles on the major tubercle in two cases, in a further case to reattach the labrum to the glenoid, whilst in a fourth only the reduction and reinforcement of the enlarged and loosened capsule was performed
Perthes, 1906;85: 199-227
1914 – Schultze describes more precisely the mechanism leading to the type of injury described by his colleagues at the previous surgical congress in 1909
Original
English
Aus den anamnestischen Erhebungen ersah ich, dass bei unsern Patienten 2 Verletzungstypen vorlagen, einerseits die Hyperabduktion — andererseits die Hyperflexion nach hinten. So hörte ich bei der Mehrzahl der Patienten, die sich noch genau auf den Vorgang bei der primären Verletzung besinnen konnten, dass sie gestolpert, vornüber gestürzt seien mit hocherhobener Hand. Während diese einen Stützpunkt suchte und sich an einen halb hohen Gegenstand im Fallen anklammerte, suchte der Stürzende unter Fixierung des Schulterblattes den Sturz aufzuhalten, kam aber doch zu Fall. Dadurch trat eine heftige Ueberstreckung im Gelenk ein. Die Kapsel kann der Gewalt nicht stand halten — sie reisst ein, es erfolgt die Luxation.
From the history I noticed that two patterns of injury were present in our patients, on the one hand hyperabduction, on the other hyperflexion towards the rear. Thus I did hear from the majority of patients that could recall precisely the events of the primary injury, that they stumbled forwards with a raised hand. As they were looking for a hold, and grabbed on to a half raised object whilst falling, the patient looked to break their fall by fixating the shoulder blade, but did fall anyways. Thereby a significant overstretching of the capsule was caused. The capsule cannot sustain this force- it tears, and the luxation follows.
1925 – Pilz first demonstrated the fact that the success or failure of the x-ray examination is dependent upon the technique used
1934 – Hermodsson reported that in many instances the defect occurred at the time of the first dislocation and did not change appreciably later, in spite of additional luxations. He reports 18 cases in which the defect was demonstrated before reduction was attempted. One of his cases was X-rayed soon after a fall from a motorcycle, and though the patient had replaced the dislocation a defect was found.
Original
English
Aus den Untersuchungen von traumatischen Verrenkungen geht hervor: teils, dass der »Defekt» schon unmittelbar nach der Verrenkung in vielen Fällen von bedeutender Grösse ist, teils, dass der Umfang der »Defekte» während der nach der Verrenkung verflossenen Zeit nicht nachweisbar gewachsen ist.
Ich will jedoch folgenden Fall erwähnen… Es handelt sich um einen Mann, der mit dem Motorrad umfiel, auf den Boden geschleudert wurde und mit dem einen Arme so aufschlug, dass dieser nach oben geschleudert wurde. Auf dem… Bilde kann man nichts anderes Bemerkenswertes finden, als einen »typischen Defekt» an dem lateralen Teile des Humeruskopfes.
In diesem Falle liegt… es nahe zur Hand, sich eine Verrenkung zu denken, die durch die eigenen Manipulationen des Patienten mit seinem Arme reponiert worden ist.
Also muss der »Defekt» durch den eigentlichen Vorgang der Verrenkung entstehen, somit ein durch die Verrenkung entstandener primärer Knochenschaden.
From the examination of traumatic dislocations it is evident: partly, that in many cases the “defect” is of considerable size already immediately following the dislocation, partly, that the diameter of the “defects” has not grown demonstrably in the time following the dislocation.
However I do wish to mention this case…It is of a man, who fell off his motorcycle, was thrown to the ground, and landed on the one arm such that it was thrust upwards. On the…image one can find nothing of note, other than a “typical defect” at the lateral part of the humeral head.
In this case one may… imagine a dislocation, that was relocated through the patient’s own manipulations.
So the “defect” must be created by the actual process of dislocation, therefore a primary bone injury
1940 – Hill and Sachs popularized the finding; provided radiographic evidence and determined a link between the presence of the lesion and persistent instability.
Incentive for this study was the discovery within a short period of time of two shoulders, each of which presented a large defect or groove in the posterolateral aspect of the head of the humerus. The defect was variously interpreted by different consultants as due to infection, metastasis, and post-traumatic osteoporosis.
…119 cases of dislocated shoulder, examined roentgenographically at the San Francisco Hospital between the years 1930 and 1940, were reviewed. This led to a clarification of our original conceptions regarding the nature of this lesion, and identified it not as a late result of dislocation of the shoulder, but as a true fracture.
Hall, Sachs 1940: 700
Hill and Sachs concluded that a minimal x-ray examination comprises an anteroposterior projection of the shoulder with the arm in adduction and external rotation and a similar projection with the arm in marked internal rotation. Below are diagrams of x-rays of the humerus in increasing degrees of rotation to illustrate the fact that only in marked internal rotation is the posterolateral aspect of the humeral head seen in profile:
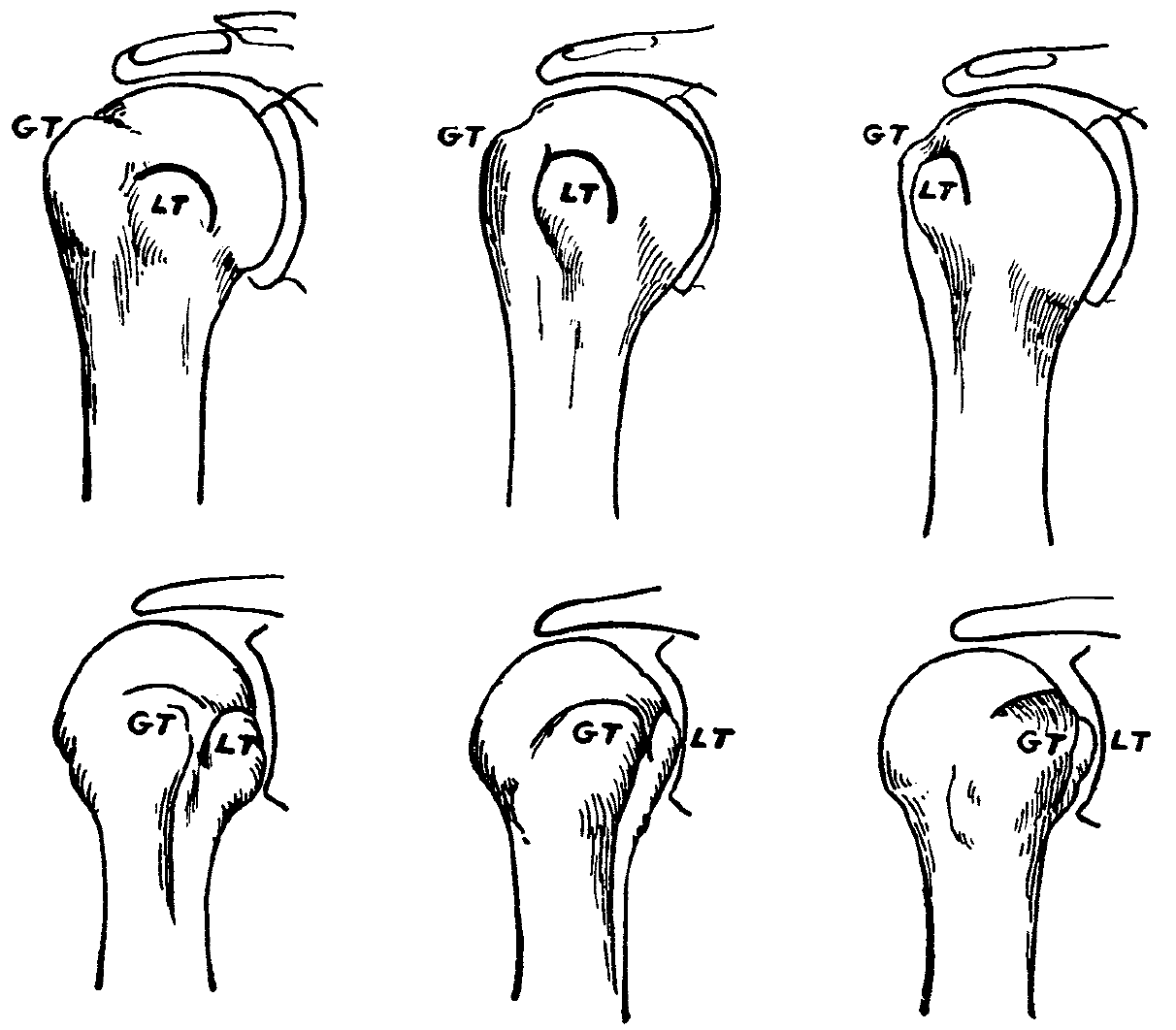
(Lower) Internal rotation of humerus: (left) moderate rotation; (center) marked; (right) very marked.
Hall, Sachs 1940: 700
A more widespread knowledge regarding the possibility of the existence of these lesions should lead to better results in the treatment of shoulder dislocations and disabilities
Hall, Sachs 1940: 700
Associated Persons
- Joseph François Malgaigne (1806 – 1865)
- Georg Clemens Perthes (1869–1927)
- Harold Arthur Hill (1901-1973)
- Maurice David Sachs (1909-1987)
Alternative names
- Hill–Sachs lesion
- Hill–Sachs fracture
- Hill–Sachs deformity
References
Historical papers
- Malgaigne JF. Chirgurue Pratique: Des Luxations scapulo-humérales. Nouveau moyens de les distinguer des fractures du col de l’humérus. Nouvelle méthode de réduction. Expériences faites à l’Hôtel-Dieu. Gazette médicale de Paris. 1832; 3(73): 506-508
- Berquet JE. Essai sur les luxations scapulo-humérales, accidentelles ou traumatiques: thèse présentée et publiquement soutenue à la Faculté de médecine de Montpellier. 1850 [Ref Malgaigne 34-35]
- Flower WH. On the Pathological Changes Produced in the Shoulder Joint by Traumatic Dislocation, as Derived from an Examination of All the Specimens Illustrating this Injury in the Museums of London. Transactions of the Pathological Society of London, 1861; 12: 179-201
- Eve FS. A Case of Subcoracoid Dislocation of the Humerus with the Formation of an Indentation on the Posterior Surface of the Head. Medico-Chirurgical Transactions, 1880; 63: 317-321.
- Perthes G. Über Operationen bei habitueller Schulterluxation. Deutsche Zeitschrift für Chirurgie. 1906; 85: 199-228
- Schultze E. Die habituellen Schulterluxationen. Archiv für klinische Chirurgie. 1914; 104: 138-179
- Pilz W. Zur Roentgenuntersuchung der Habituellen Schulterverrenkung. Archiv für klinische Chirurgie 1925; 135: 1-22
- Hermodsson I. Rontgenologische Studien ueber die traumatischen und habituellen Schultergelenkverrenkungen nach vorn und nach unten. Acta radiologica supplementum. 1934; 20: 1-173
- Hill HA, Sachs MD. The grooved defect of the humeral head: a frequently unrecognized complication of dislocations of the shoulder joint. Radiology. 1940; 35(6): 690–700
Review of the Hills-Sachs deformity
- Calandra JJ, Baker CL, Uribe J. The incidence of Hill-Sachs lesions in initial anterior shoulder dislocations. Arthroscopy. 1989; 5(4): 254-7
- Cetik O, Uslu M, Ozsar BK. The relationship between Hill-Sachs lesion and recurrent anterior shoulder dislocation. Acta Orthop Belg. 2007; 73(2): 175-178.
- Gyftopoulos S, Albert M, Recht MP. Osseous injuries associated with anterior shoulder instability: what the radiologist should know. AJR Am J Roentgenol. 2014; 202(6): W541-550.
- Somford MP, Nieuwe Weme RA, van Dijk CN, IJpma FF, Eygendaal D. Are eponyms used correctly or not? A literature review with a focus on shoulder and elbow surgery. Evid Based Med. 2016; 21(5): 163-71
- Somford MP, Van der Linde JA, Wiegerinck JI, Hoornenborg D, Van den Bekerom MPJ, Van Deurzen DFP. Eponymous terms in anterior shoulder stabilization surgery. Orthop Traumatol Surg Res. 2017; 103(8): 1257-1263.
eponymictionary
the names behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
