
![]()
CT Case 105
A 69 year old male presents with two days of atraumatic progressively worsening neck and scalp pain. He has a background of type II diabetes mellitus and chronic kidney disease.
On examination he has marked reduced range of motion of his cervical spine in all directions. He has hyperalgesia of his scalp, occiput, and posterior neck. He has no objective neurological deficit.
His bloods showed an elevated CRP (80) and ESR (50).
A CT of his cervical spine is arranged.
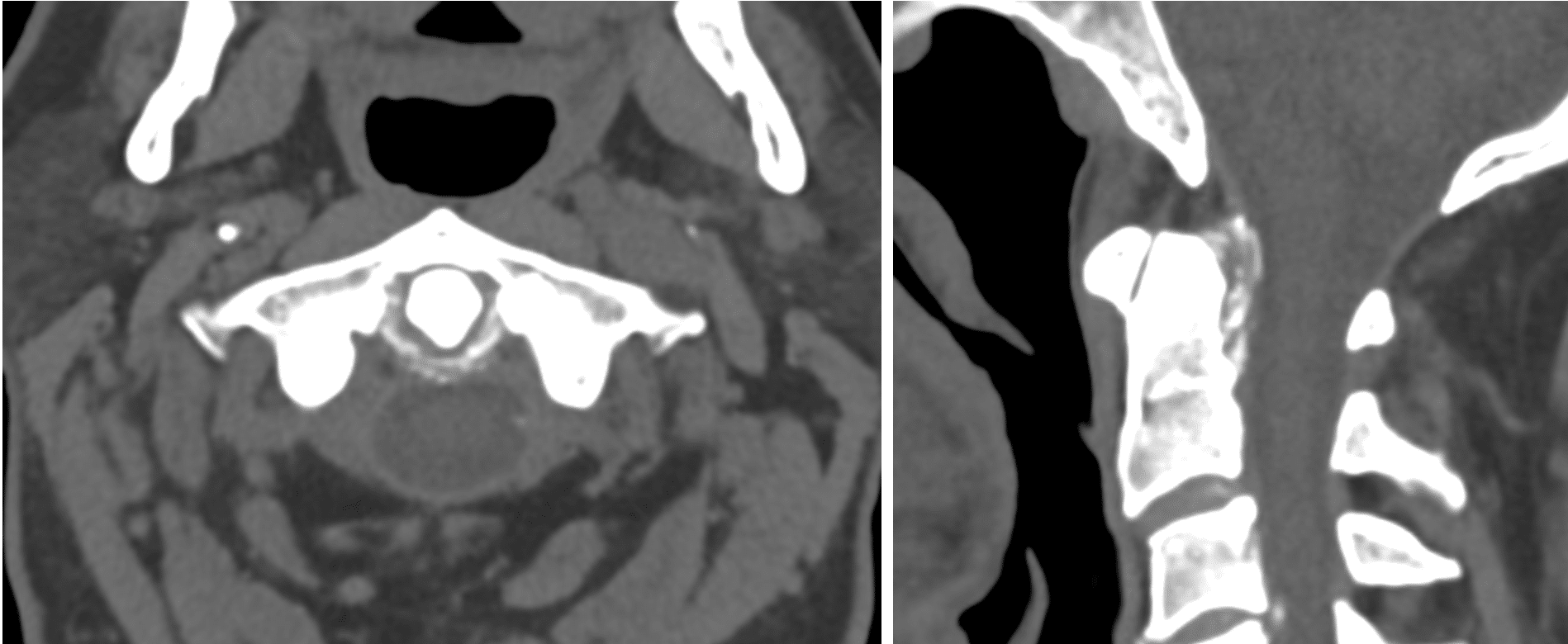
Describe and interpret the CT scan
There is partial periodontal ligament calcification involving the superior, transverse and inferior fibres of the cruciform ligament as well as the alar ligament.
There is mild subchondral sclerosis of the anterior atlantoaxial joint.
High density material around atlantodental interval
Erosion at posterior tip
Widening of the clival odontoid tip
No acute cervical spine fracture.
Satisfactory bony alignment of the craniocervical junction.
No gross cervical spinal malalignment.
Conclusion: Periodontal ligament calcification as described which can be seen in crowned dens syndrome in the appropriate clinical and biochemical context.
Clinical Pearls
This CT is supportive of a diagnosis of crowned dens syndrome.
Crowned dens syndrome is a rare condition caused by the deposition of calcium pyrophosphate dihydrate crystals around the odontoid process of C2.
Patients present with acute neck pain, stiffness, fevers, and elevated inflammatory markers (1). The onset is more often acute than insidious, and the syndrome occurs most commonly in patients older than 60 with a predisposition for females (2). If left untreated, this condition may lead to chronic neck pain, spinal cord compression, or fractures of the odontoid process (3, 4). It remains unclear if this condition is associated with other crystal deposition diseases (5, 6).
The diagnosis is based on clinical findings and imaging, with CT being the gold standard of diagnosis. CT identifies calcification of periodontal ligaments, particularly the transverse ligament of the atlas (3).
Treatment is centred around NSAIDs, corticosteroids, colchicine, or combination therapy (1). The prognosis is generally good with the majority of patients fully recovering within a few weeks of treatment being commenced (7).
This patient was briefly admitted under the rheumatology team and treated with a weaning course of prednisone and colchicine. His symptoms improved and he was discharged with outpatient follow up.
References
- Tajima K, Ueda T, Ueno K, Shimizu C, Yoshizawa J, Hori S. Crowned dens syndrome: reports of six cases and review of the literature. Acute Med Surg. 2015 Aug 12;3(2):155-158.
- Siau K, Lee M, Laversuch CJ. Acute pseudogout of the neck–the crowned dens syndrome: 2 case reports and review of the literature. Rheumatol Int. 2011 Jan;31(1):85-8.
- Aouba A, Vuillemin-Bodaghi V, Mutschler C, De Bandt M. Crowned dens syndrome misdiagnosed as polymyalgia rheumatica, giant cell arteritis, meningitis or spondylitis: an analysis of eight cases. Rheumatology (Oxford). 2004 Dec;43(12):1508-12.
- Kakitsubata Y, Boutin RD, Theodorou DJ, Kerr RM, Steinbach LS, Chan KK, Pathria MN, Haghighi P, Resnick D. Calcium pyrophosphate dihydrate crystal deposition in and around the atlantoaxial joint: association with type 2 odontoid fractures in nine patients. Radiology. 2000 Jul;216(1):213-9.
- Roverano S, Ortiz AC, Ceccato F, Paira SO. Calcification of the transverse ligament of the atlas in chondrocalcinosis. J Clin Rheumatol. 2010 Jan;16(1):7-9.
- Sekijima Y, Yoshida T, Ikeda S. CPPD crystal deposition disease of the cervical spine: a common cause of acute neck pain encountered in the neurology department. J Neurol Sci. 2010 Sep 15;296(1-2):79-82
- Goto S, Umehara J, Aizawa T, Kokubun S. Crowned Dens syndrome. J Bone Joint Surg Am. 2007 Dec;89(12):2732-6.
TOP 100 CT SERIES

FACEM, MBBS (Hon), B. Pharm. Emergency Medicine Education Fellow at Liverpool Hospital, Australia. Special interests in clinical education, ECG interpretation and diagnostic ultrasound. Proud father and husband, sadly a golf tragic

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney