
![]()
CT Case 106
A 70 year old woman presents with 12 hours of lower abdominal pain and one episode of haematochaezia at home. She has a background of hypertension and takes no anticoagulant or antiplatelet agents.
On exam she appears well and vital signs show HR 105/min and BP 170/90mmHg with no fever. Her abdomen is soft with mild left lower quadrant tenderness. She is cannulated and bloods sent off. Shortly after presentation the patient has a syncopal event and her BP drops to 70mmHg. She is found to have lost a large volume of blood per rectum (approximately 700mL).
The patient is sent for an urgent CT mesenteric angiogram.
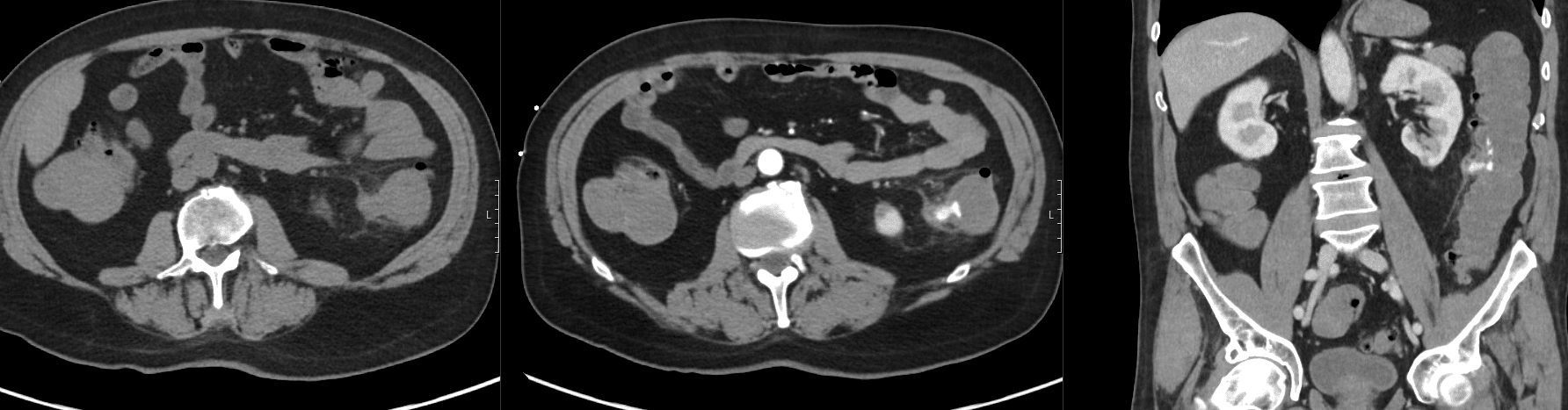
Describe and interpret the CT scan
There is arterial blush and portal venous pooling involving an inflamed diverticulum in the descending colon.
Heterogeneous relatively high density fluid throughout the colon and rectum, likely blood products. There is pericolic fat stranding and free fluid.
No extraluminal gas or peripherally enhancing collection.
Extensive background colonic diverticulosis.
This CT demonstrates an acute colonic diverticular bleed.
Clinical Pearls
This CT demonstrates an acute colonic diverticular bleed.
Colonic diverticular bleeds are the most common cause of haematochezia (1). The right colon is the most common site of bleeding which is in contrast to the most common site of diverticulitis which is the left side of the colon. The cause of bleeding is thought to be due to thinning of the media of the wall of the colonic vessel as it is draped over the dome of the herniated diverticulum; these changes result in a segmental weakness of the artery eventually resulting in rupture into the lumen of the colon. Right sided diverticula tend to have wider necks and domes which expose a greater length of the colonic vessels to injury compared to the left side (2).
The risk of bleeding in patients with asymptomatic diverticulosis is low with a bleeding incidence rate of approximately 0.2% per year (3). It is important to note that it is rare for patients with diverticular bleeds to simultaneously have diverticulitis.
Diagnosis of colonic diverticular bleeds depends on the severity of bleeding. Colonoscopy is the best imaging modality for the majority of patients and allows for therapeutic intervention to be performed at the same time via clips, ligation, or thermal therapy.
CT angiography is preferred for patients with severe persistent bleeding resulting in haemodynamic instability despite volume resuscitation. Active bleeding is required to identify a bleeding source with a rate of blood loss exceeding 0.35mL/min. The sensitivity of CT angiography in the localisation of gastrointestinal is approximately 90% when there is active bleeding, with detection rates falling to 45% when the bleeding is intermittent (3). Angiographic treatment is more likely to be successful if it is performed within 90 minutes of a positive CT angiogram and involves transcatheter embolization of the bleeding site via microcatheters. Surgery may be indicated for bleeding that can not be controlled with angiographic or endoscopic intervention. This patient was resuscitated with blood products while discussions were had with the general surgical team and interventional radiologist (IR).
The patient was investigated by IR with direct angiography of the inferior mesenteric artery which did not find any vascular abnormality or active haemorrhage, and thus embolization was not performed. The patient was monitored by the colorectal surgical team for 4 days and had no further bleeds so was discharged with outpatient colonoscopy arranged.

References
- Ghassemi KA, Jensen DM. Lower GI bleeding: epidemiology and management. Curr Gastroenterol Rep. 2013 Jul;15(7):333.
- Imbembo AL, Bailey RW. Diverticular disease of the colon. In: Textbook of Surgery, 14th ed, Sabiston DC Jr (Ed), Churchill Livingstone, 1992: 910.
- Niikura R, Nagata N, Shimbo T, Aoki T, Yamada A, Hirata Y, Sekine K, Okubo H, Watanabe K, Sakurai T, Yokoi C, Mizokami M, Yanase M, Akiyama J, Koike K, Uemura N. Natural history of bleeding risk in colonic diverticulosis patients: a long-term colonoscopy-based cohort study. Aliment Pharmacol Ther. 2015 May;41(9):888-94.
TOP 100 CT SERIES

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney

FACEM, MBBS (Hon), B. Pharm. Emergency Medicine Education Fellow at Liverpool Hospital, Australia. Special interests in clinical education, ECG interpretation and diagnostic ultrasound. Proud father and husband, sadly a golf tragic
