
![]()
Diagnosis, Wenckebach Squared?
aka ECG Exigency 018.2
Thanks to all who contributed to solving the puzzle of Diagnosis, Wenckebach? in ECG Exigency 018.1 – Let’s recap:
The following tracing can be found in our ECG library, allegedly as an example of Wenckebach AV block. However, as one of our readers, Jan Štros has pointed out, there is something not entirely right about this ECG tracing…Can you spot the ‘deliberate’ mistake?
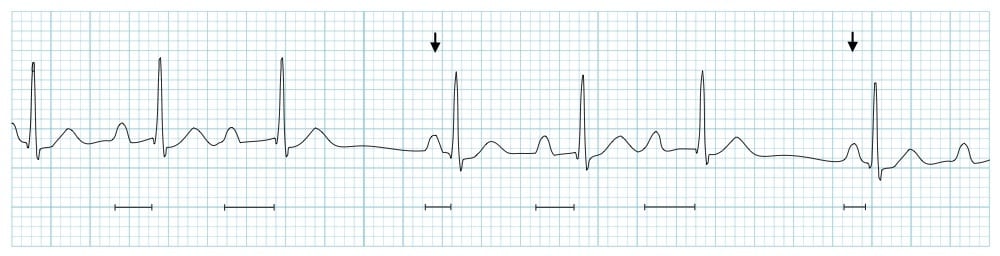
- Q1. What features of Wenckebach AV block are present on this ECG?
- Q2. What features of Wenckebach are notably ABSENT?
- Q3. What possible explanations could exist to explain this tracing?
Here is my impression of the ECG (by no means the “correct” answers) is as follows…
Q1. What features of Wenckebach AV block are present on this ECG?
Answer and Interpretation
Answer:
- The presence of a progressively prolonging PR interval that abruptly shortens (i.e. resets) after a pause in the rhythm is strongly suggestive of Wenckebach AV block.
Explanation:
- The underlying process is progressive fatigue of dysfunctional AV node cells. Commonly, this culminates in a non-conducted P wave, as the AV node cells fatigue to the point where they are unable to conduct a further impulse.
- However, anything that interrupts the rhythm (e.g. a sinus pause or ventricular ectopic beat) will give the AV node cells chance to “rest”, following which they will conduct normally.
Q2. What features of Wenckebach are notably ABSENT?
Answer and Interpretation
Answer:
- Notably absent is the lack of a non-conducted P wave. While it is tempting to assume (as I did) that the non-conducted P wave must be hidden in the preceding T wave, there is no evidence of this – the P waves are too tall to be superimposed on the T waves without producing an obvious “bump”.
Explanation:
- As discussed above, the presence of a non-conducted P wave is not required to make the diagnosis of Wenckebach AV block.
Q3. What possible explanations could exist to explain this tracing?
Answer and Interpretation
Answer:
The frequently dropped P waves occurring in a regular pattern are suggestive of second degree SA block (type I). Features that are supportive of this:
- Grouping of the QRS complexes
- The duration of the each sinus pause is less than double the preceding PP interval
Explanation:
There are two types of cells in the SA node – the inner core of P cells that produce the impulse, and the outer layer of T cells that transmit the impulse out into the atrium. Analogous to Wenckebach AV block, progressive fatigue of the T cells produces second-degree SA exit block (type I), also known as Wenckebach SA block.
This is the most common type of SA block detectable on the surface ECG and is characterized by grouping / clustering of the QRS complexes culminating in a dropped P wave.
See our ECG library page on SA block for further explanation.
Final Interpretation
Possible causes of this ECG pattern would include conditions that suppress both SA and AV node function, e.g.
- Sick sinus syndrome
- Increased vagal tone
- Inferior AMI
- Myocarditis
- Drugs: digoxin, beta-blockers, Ca channel blockers
So, the final diagnosis:
Wenckebach AV block with Wenckebach SA block!
References
- Burns E. Diagnosis, Wenckebach?
- Burns E. Block: Mobitz 1 Wenkebach
- Hampton, JR. The ECG In Practice, 6e
- Mattu A, Brady W. ECG’s for the Emergency Physician 1
- Mattu A, Brady W. ECGs for the Emergency Physician 2
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric, 6e
- Wagner, GS. Marriott’s Practical Electrocardiography 12e
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF

CLINICAL CASES
ECG EXIGENCY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |
I do have another ECG with the same finding, and I do agree with you for the diagnosis of Wenckebach AV block with Wenckebach SA block
It is simultaneous SA Mobitz I and AV Mobitz I. The conduction ratio of the SA/atrium interface is less than the conduction ratio of the AV node. So, when the the SA node reaches the end of its episode, it blocks and the entire pathway from SA node to the last ventricular myocyte has time to repolarize and then start over again. The AV Mobitz I never gets the opportunity to reveal its actual conduction ratio.
The P-P interval remains unchanged meaning the SA impulse is not progressively stalled. Constant P-P interval so would this rather be a Wenkebach AV block with Second Degree SA Mobitz II instead?
If this SA second degree type 2, the P wave will has an exact multiple of the preceding P-P interval