![]()
Beta-blocker and Calcium-channel blocker toxicity
Relevant agents
- Beta-blockers: Atenolol, metoprolol, propranolol, sotalol
- Cardioselective calcium-channel blockers: Verapamil and diltiazem
Effects on the ECG
- Sinus bradycardia
- 1st degree, 2nd degree and 3rd degree AV block
- Junctional bradycardia
- Ventricular bradycardia
A prolonged PR interval is an early sign of beta-blocker or calcium-channel blocker toxicity — even in the absence of significant bradycardia.
Specific Agents
Two beta-blockers have additional important toxic effects:
Propanolol:
- Propranolol behaves more like a tricyclic antidepressant in overdose than a beta-blocker, due to its blockade of myocardial and CNS fast sodium channels
- Propranolol toxicity is associated with QRS widening and a positive R’ wave in aVR (signs of sodium channel blockade), which portend the onset of coma, seizures, hypotension and ventricular arrhythmias
Sotalol
- Sotalol blocks myocardial potassium channels, causing QT prolongation and Torsades de Pointes in overdose
ECG Examples
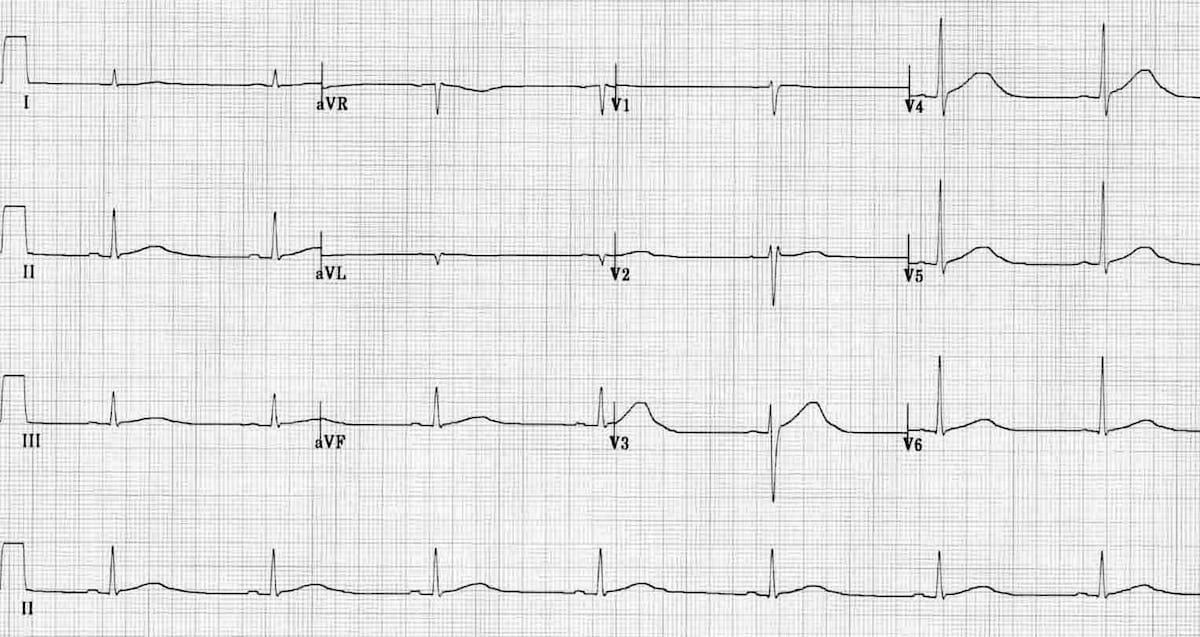
Example 1
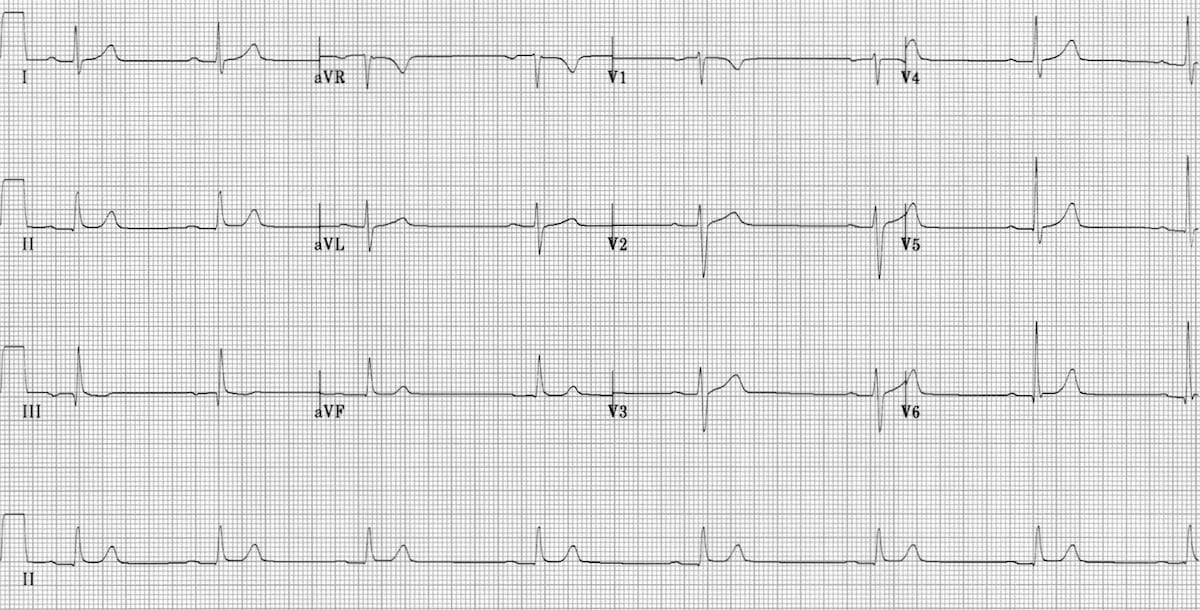
Sinus bradycardia with 1st-degree AV block:
- Heart rate 45 bpm
- PR interval 240 ms
This type of ECG pattern is commonly seen in the early stages of beta-blocker / calcium-channel blocker poisoning.
Example 2
Slow junctional rhythm:
- Regular rhythm at 30 bpm
- Narrow QRS complexes
- No visible P waves
Example 3
Complete heart block:
- Sinus rhythm – P waves occur at a rate of around 90 bpm
- 3rd degree AV block – there is no relationship between the P waves and QRS complexes
- Slow escape rhythm (30 bpm) with a RBBB morphology – this could be either a ventricular escape rhythm or a slow junctional rhythm with RBBB
Example 4
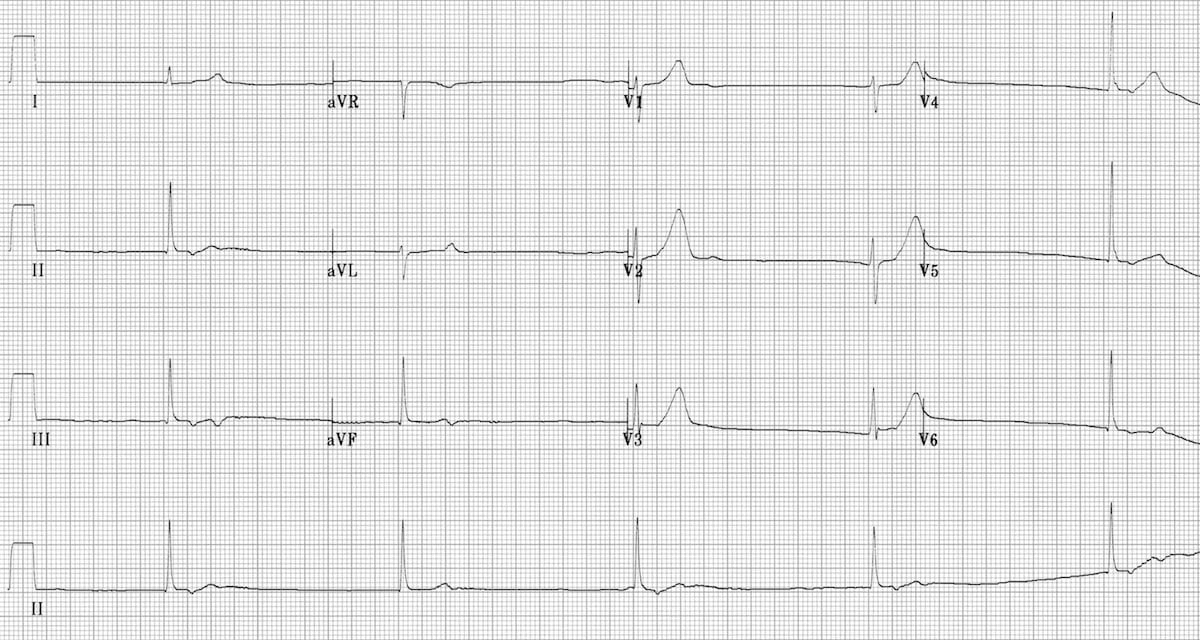
This ECG demonstrates the key features of sotalol overdose:
- Sinus bradycardia
- Very long QT interval (~600ms)
NB. This patient is at significant risk of Torsades de Pointes.
Example 5
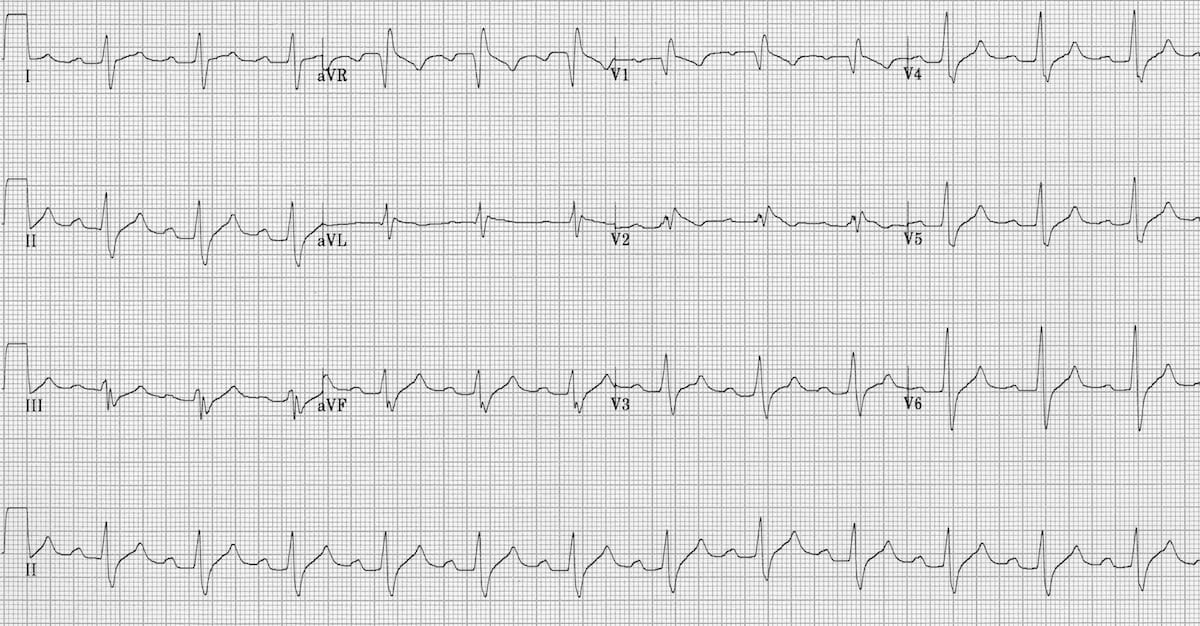
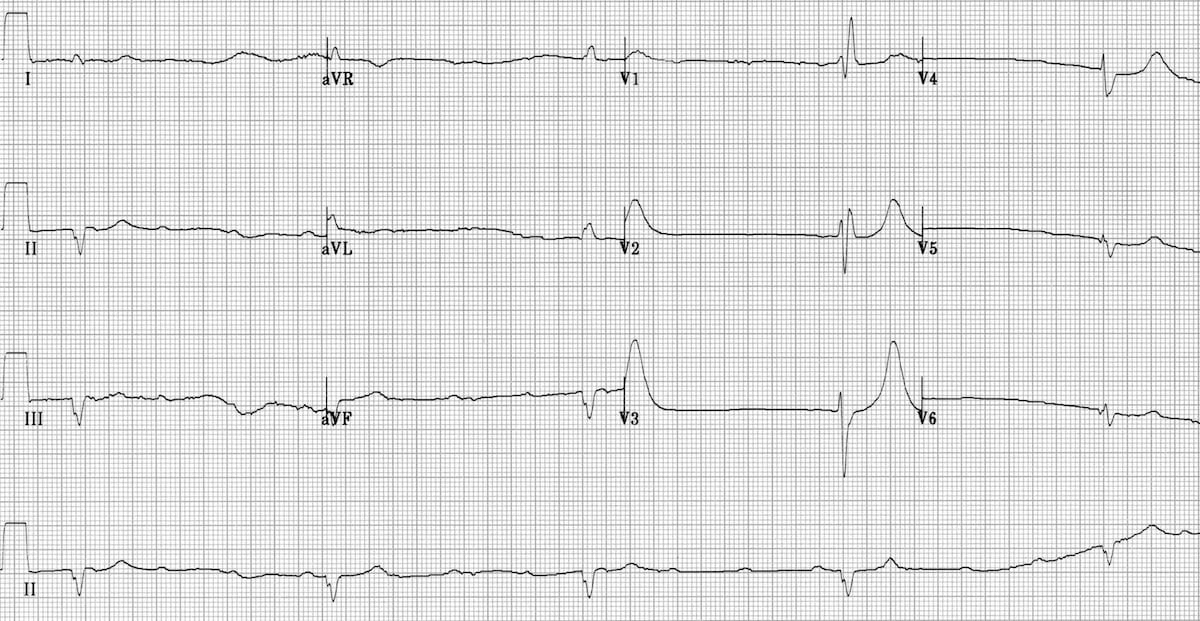
This ECG demonstrates some of the key features of propranolol overdose:
- 1st degree AV block
- Signs of sodium-channel blockade: QRS broadening (> 100 ms) and positive R’ wave in aVR (> 3mm)
NB. Normally the heart rate would be slower than this in a propranolol overdose (this is actually an ECG of flecainide poisoning — another sodium-channel blocking agent).
Related Topics
- Tricyclic antidepressant overdose (sodium-channel blocker toxicity)
- Digoxin toxicity
- Carbamazepine toxicity
- Quetiapine toxicity
References
- Dr Smith’s ECG Blog – Differential diagnosis of severe bradycardia (case discussions)
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.