
![]()
Sinoatrial Exit Block
SA Exit Block Overview
Sinoatrial exit block is due to failed propagation of pacemaker impulses beyond the SA node.
- The sinoatrial node continues to depolarise normally.
- However, some of the sinus impulses are “blocked” before they can leave the SA node, leading to intermittent failure of atrial depolarisation (dropped P waves).
Anatomical Basis
The SA node consists of two main groups of cells:
- A central core of pacemaking cells (P cells) that produce the sinus impulses.
- An outer layer of transitional cells (T cells) that transmit the sinus impulses out into the right atrium.
Sinus node dysfunction can result from either:
- Failure of the P cells to produce an impulse. This leads to sinus pauses and sinus arrest.
- Failure of the T cells to transmit the impulse. This leads to sino-atrial exit block.
Patterns of conduction
- The patterns of conduction in SA exit block are identical to the different types of AV block.
- However, as the initial sinus impulse is not visible on the ECG, the relationship between impulse generation and transmission must be inferred from the P waves alone (analogous to examining only the R waves in AV block).
- Only second degree SA block (types I and II) can be diagnosed from the 12-lead ECG.
First Degree SA block
= Delay between impulse generation and transmission to the atrium.
- This abnormality is not detectable on the surface ECG.
Second Degree SA block, Type I (Wenckebach)
= Progressive lengthening of the interval between impulse generation and transmission, culminating in failure of transmission.
- The gradually lengthening transmission interval pushes successive P waves closer together.
- This results in grouping of the P-QRS complexes.
- Pauses due to dropped P waves occur at the end of each group.
- The P-P interval progressively shortens prior to the dropped P wave.
- This pattern is easily mistaken for sinus arrhythmia.
Second Degree SA block, Type II
= Intermittent dropped P waves with a constant interval between impulse generation and atrial depolarisation.
- This pattern is the equivalent of Mobitz II.
- There is no clustering of P-QRS complexes.
- Intermittent P waves “drop out” of the rhythm, while subsequent P waves arrive “on time”.
- The pause surrounding the dropped P wave is an exact multiple of the preceding P-P interval.
Third Degree SA Block
= None of the sinus impulses are conducted to the right atrium.
- There is a complete absence of P waves.
- The onset of 3rd degree SA block may produce long sinus pauses or sinus arrest (may lead to fatal asystole).
- Rhythm may be maintained by a junctional escape rhythm.
- Third degree SA exit block is indistinguishable from sinus arrest due to pacemaker cell failure. It can only be diagnosed with a sinus node electrode during electrophysiological evaluation.
Causes of sinoatrial exit block
- Sick sinus syndrome
- Increased vagal tone (athletes)
- Vagal stimulation (surgery, pain)
- Inferior myocardial infarction
- Myocarditis
- Drugs: digoxin, beta-blockers, calcium channel blockers, amiodarone.
ECG Examples
Example 1

Type I SA block
- This pattern of grouped beating is characteristic of type I SA block.
- There is progressive shortening of the P-P interval, followed by an absent P wave-QRS complex.
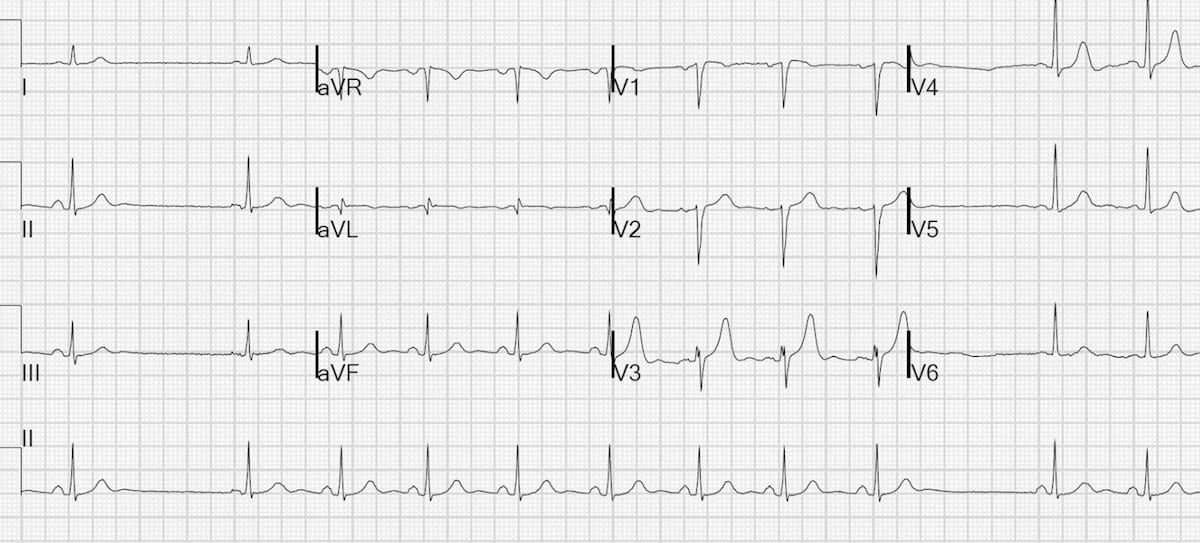
Example 2

Type II SA block
- Arrows indicate the presumed timing of each sinus impulse.
- The blue arrows represent normally transmitted impulses, i.e. resulting in P waves.
- The black arrows represent blocked sinus impulses (dropped P waves).
- The pauses around the dropped P waves (2.1 seconds) are exactly double the preceding P-P interval (1.05 seconds)
Also note:
- The 4th QRS complex is a junctional escape beat followed by a non-conducted P wave (occurring just prior to the T wave).
- The 8th QRS complex is a junctional escape beat. The following P wave is conducted to the ventricles, albeit with an extremely long PR interval (400ms).
Image Credit: Dr Steve Smith’s ECG Blog
Related Topics
- Clinical Case: “Wenckebach Squared!” A case of simultaneous SA exit block and AV Mobitz I block
- AV block: 1st degree
- AV block: 2nd degree, Mobitz I (Wenckebach)
- AV block: 2nd degree, Mobitz II
- AV block: 3rd degree (complete heart block)
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.