
![]()
Dix-Hallpike Manoeuvre
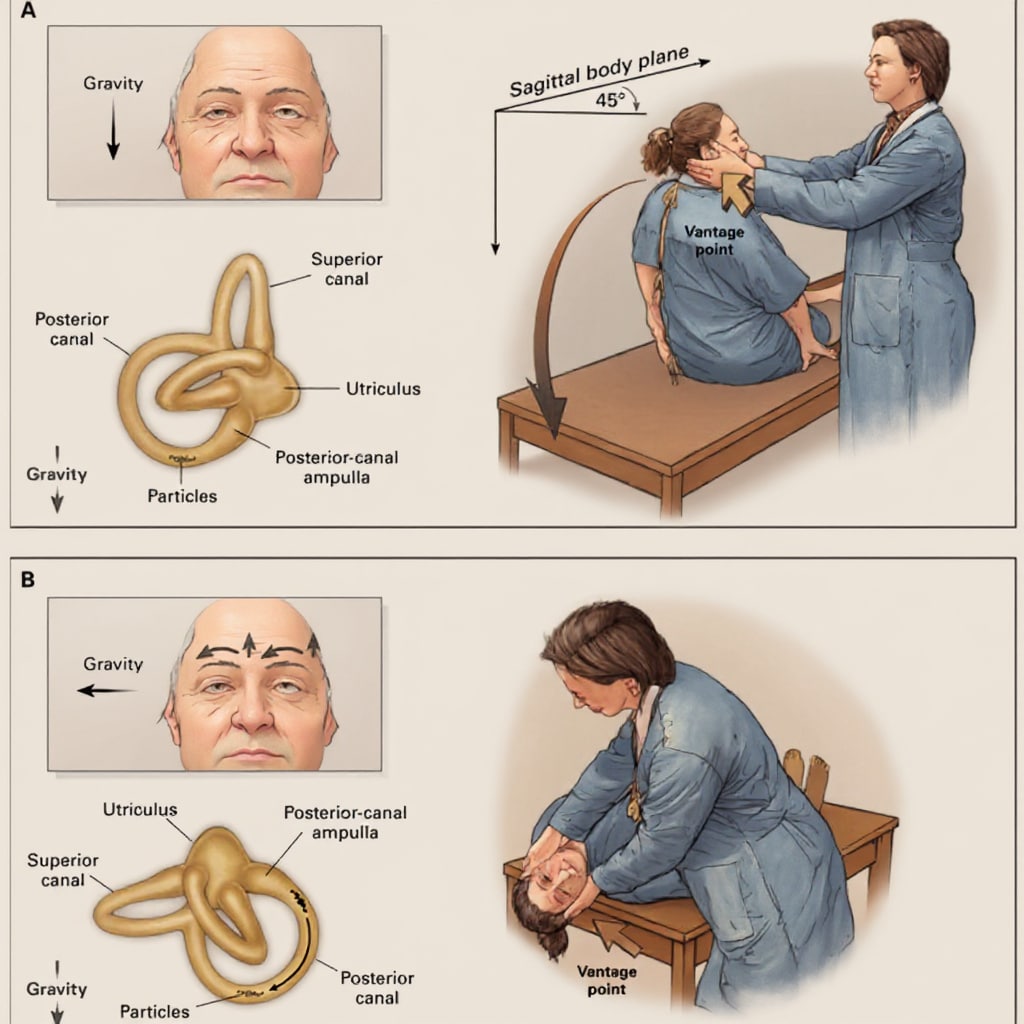
The Dix-Hallpike manoeuvre is the gold standard test for the diagnosis of posterior semicircular canal benign paroxysmal positional vertigo (BPPV), first described by Dix and Hallpike in 1952. It is used to elicit positional vertigo and characteristic nystagmus associated with BPPV.
- Purpose: Differentiates posterior canal BPPV from other causes of vertigo.
- Mechanism: Displaces otolith debris in the posterior semicircular canal, triggering vertigo and nystagmus due to inappropriate stimulation of vestibular hair cells.
Technique:
- Explain the procedure and reassure the patient. Warn about potential vertigo and nausea.
- Position the patient seated on the examination couch, legs extended.
- Turn the head 45° toward the side being tested.
- Rapidly lower the patient to a supine position with the head extended ~20° below horizontal, hanging off the edge of the bed.
- Observe the eyes for torsional and vertical nystagmus, typically delayed by 2–5 seconds.
- After ~30 seconds or once symptoms resolve, return the patient to sitting.
Positive test: Upbeat-torsional nystagmus and reproduction of vertigo symptoms. Nystagmus usually fatigues with repetition and is transient (<1 minute).
Clinical nuances:
- If the first test is negative but clinical suspicion remains, repeat the test after a short rest. Up to 10–20% of patients with true BPPV may only show positive findings on repeat testing.
- The non-affected side is often tested first to familiarise the patient and mitigate anticipatory anxiety.
- Patients should keep their eyes open, and if available, Frenzel goggles can enhance nystagmus detection.
- Contraindications include severe cervical spine disease, recent neck trauma, or vertebrobasilar insufficiency.
Sensitivity and limitations:
- Reported sensitivity ranges from 48–88% for posterior canal BPPV.
- Visual fixation may suppress nystagmus—watch the patient’s eyes closely and avoid letting them fixate on an object.
Video: Dix-Hallpike in practice
Transcript
- Diagnostic test, used when you suspect benign paroxysmal positional vertigo
- Explain the procedure to the patient, and warn them that they may experience vertigo symptoms during it, but that the symptoms usually subside quickly.
- NOTE: Check that the patient does not have any neck injuries or other contraindications to rapid spinal movements
- NOTE: signs and symptoms usually occur when you turn the patient’s head towards the lesion, so if you suspect disease of the right ear, you may wish to start on their right side – the non-affected side
- Ask the patient to keep their eyes open throughout and stare at your face.
- Have them sit on an examination bed with their legs extended, close enough to the edge so that their head will hang over when they are laid flat.
- Stand on their left side. Take hold of their head with both hands, and turn their head 45° towards you (tests the left posterior canal). Observe their eyes for 30 seconds
- Keeping the patient’s head in the same position, lie them down quickly until their head is hanging over the edge of the couch (still turned 45° towards you). Observe their eyes for 30 seconds.
- Lift the patient back up to sitting position, and repeat the test on their right side
In a patient with BPPV, you will typically see a characteristic pattern of nystagmus emerge after 5-20 seconds, when the patient’s head is hanging towards the side of the lesion. This is torsional or rotatory nystagmus and has two components: a quick movement towards the side of the lesion and a slow component away from it. An upward beating nystagmus is often superimposed on this movement.
History
1952 – Margaret Ruth Dix (1911-1991) and Charles Skinner Hallpike (1900-1979) published a landmark paper in neuro-otology, looking at the three most common peripheral vertigo diseases: Menière’s disease, vestibular neuritis and benign paroxysmal positional vertigo.
In their landmark 1952 paper, Dix and Hallpike provided the first detailed description of what they termed the Lagerungs (positioning) manoeuvre, writing:
The patient is laid supine upon a couch with his head just over its end. The head is then lowered some 30 degrees below the level of the couch and turned some 30 degrees to 45 degrees to one side. In taking up this position, the patient is first seated on the couch with the head turned to one side and the gaze fixed upon the examiner’s forehead. The examiner then grasps the patient’s head firmly between his hands and briskly pushes the patient back into the critical position.
Dix and Hallpike, 1952
Dix–Hallpike Manoeuvre: Original vs. Modern Interpretation
| Aspect | Dix & Hallpike, 1952 (Original Description) | Modern Clinical Criteria |
|---|---|---|
| Patient position | “The patient is seated on the couch with the head turned 30–45° to one side, gaze fixed on the examiner’s forehead… The examiner then briskly pushes the patient back, so the head lies 30° below horizontal, over the end of the couch.” | Patient starts sitting upright; head is rotated 45° toward test side; patient rapidly lowered to supine with head hanging 20–30° below horizontal. |
| Provocation | Rapid change in head position relative to gravity (Lagerungs manoeuvre). | Same principle; diagnostic for posterior canal BPPV. |
| Nystagmus observed | Rotatory nystagmus beating toward the undermost ear, after a short latency, with fatigability on repetition. | Posterior canal: torsional upbeat nystagmus with 2–15 sec latency; fatigues with repetition; reversal on sitting up. |
| Interpretation | Described as “positional vertigo of the benign paroxysmal type.” | Standard diagnostic test for BPPV; allows canal-specific localisation (posterior > lateral > anterior). |
| Clinical impact | First systematic clinical–physiological correlation of vertigo with head positioning; established reproducible manoeuvre for research and practice. | Remains the gold standard bedside test; used worldwide; essential for guiding repositioning treatments (Epley, Semont, etc.). |
Associated Persons
- Róbert Bárány (1876-1936)
- Margaret Ruth Dix (1911-1991)
- Charles Skinner Hallpike (1900-1979)
Alternative names
- Lagerungs Manoeuvre
References
Historic references
- Bárány R. Die nervosen Storungen des Cochlear- und Vestibularapparates. In: Handbuch der Neurologie [Lewandowsky M (ed.)] 1910; I(IV): 919-958
- Dix MR, Hallpike CS. The pathology symptomatology and diagnosis of certain common disorders of the vestibular system. Proc R Soc Med. 1952; 45(6): 341-54
- Dix MR, Hallpike CS. The pathology, symptomatology and diagnosis of certain common disorders of the vestibular system. Ann Otol Rhinol Laryngol. 1952; 61(4): 987-1016.
eponymictionary
the names behind the name

Studied at Univerisity of Cambridge - BA MB BChir. British doctor working in emergency medicine in Perth, Australia. Special interests include primary care and emergency medicine.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |