
![]()
ECG Case 056
Middle-aged patient presenting with drowsiness. Brief seizure in ED. BP unrecordable. Interpret the ECG.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
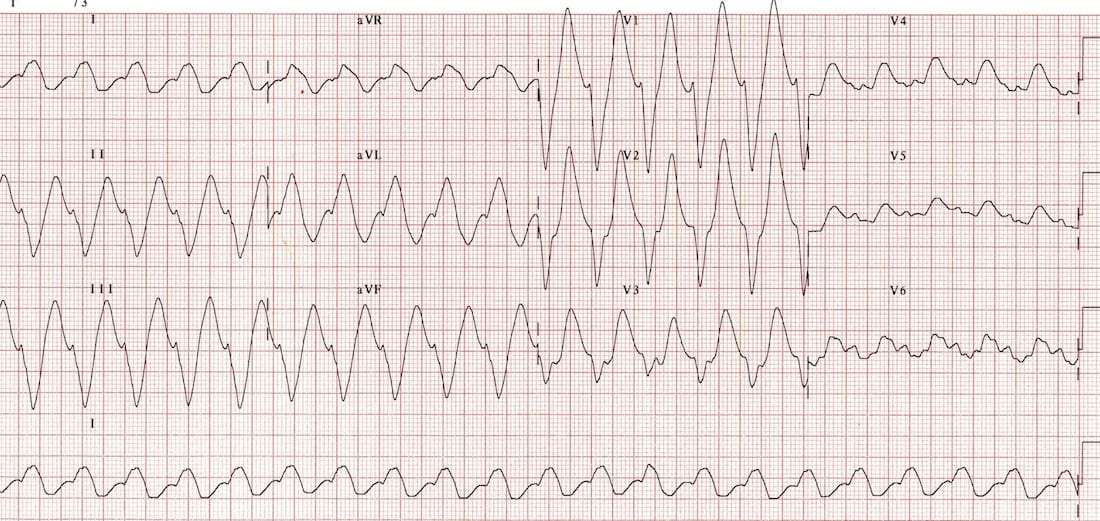
This is a repeat ECG of the previous patient with massive TCA overdose, taken a short while later.
- There is now evidence of advanced sodium-channel blockade, with grossly prolonged QRS and QT intervals and further evolution of the R’ wave in aVR.
- The ECG is beginning to take on bizarre morphology and a sine wave appearance reminiscent of severe hyperkalaemia.
- In some leads (II, III, aVF), the QRS morphology resembles ventricular tachycardia.
These features are all due to sodium-channel blockade, and resolved following aggressive treatment with IV bicarbonate, intubation and hyperventilation.
Post-treatment ECG
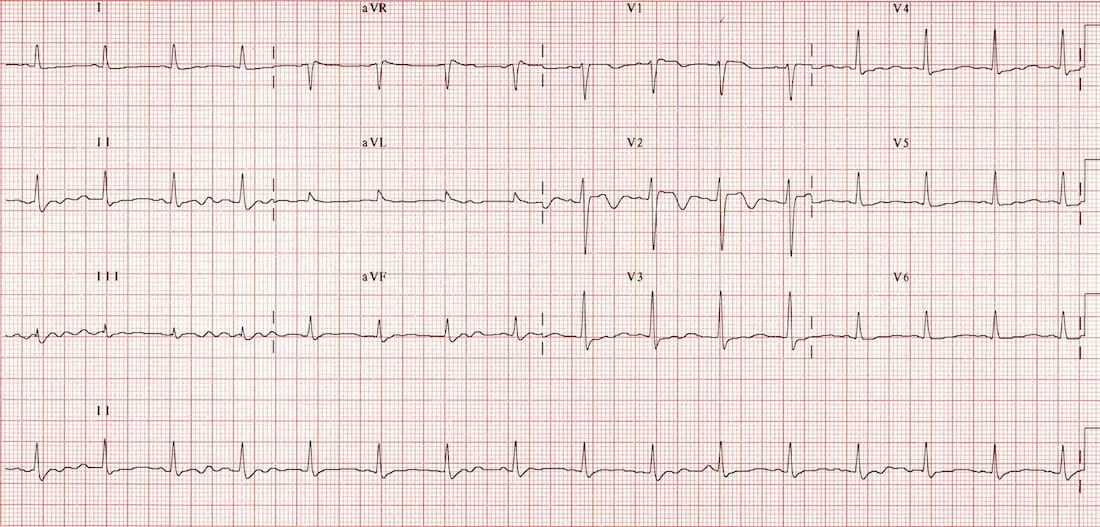
Resolving TCA toxicity – QRS complexes narrowing and R’ wave disappearing with treatment.
CLINICAL PEARLS
Advanced sodium-channel blockade can resemble either VT or hyperkalaemia.
Standard VT treatments such as DC cardioversion and amiodarone are likely to be ineffective and potentially harmful if the broad complex rhythm is due to sodium-channel blockade. Consider the clinical context and look for clues of TCA toxicity (e.g. anticholinergic toxidrome).
In arrested / peri-arrest patients with a broad or bizarre-looking ECG, consider empirical treatment for both hyperkalaemia (with calcium) and sodium-channel blockade (with bicarbonate and hyperventilation).
References
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 100 ECG Series
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |