
![]()
ECG Case 072
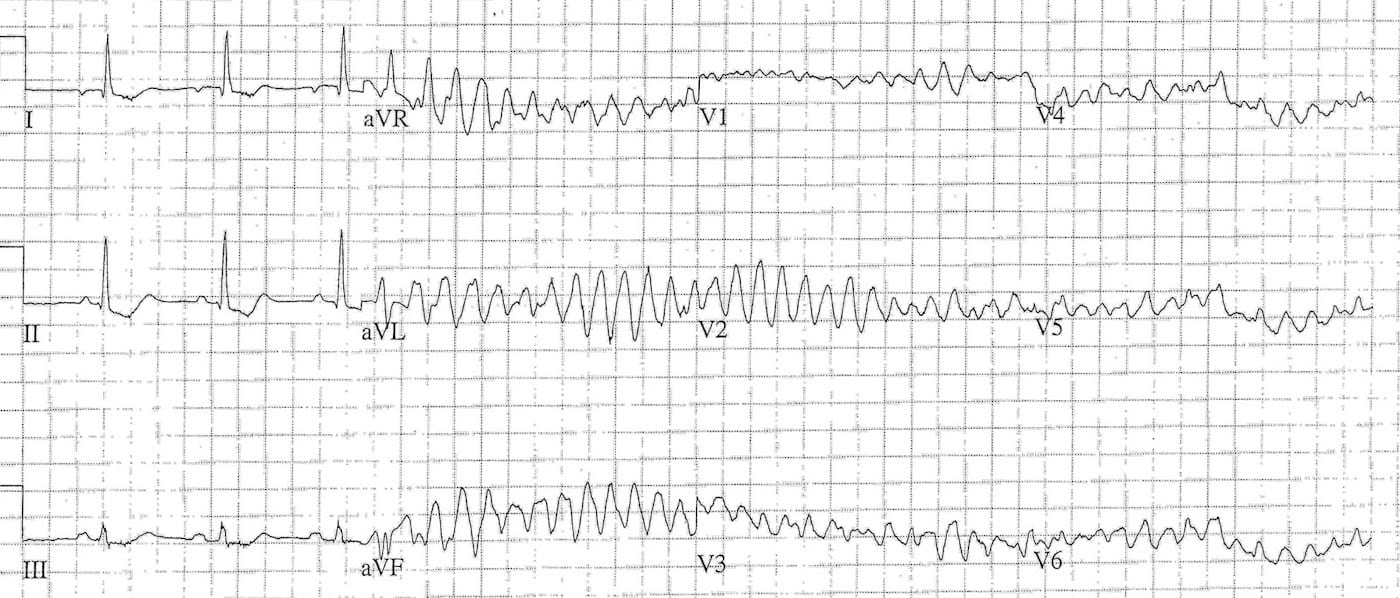
This ECG is from a 49 year old. He self-presented to the emergency department with chest pain, initial ECG is below.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Initial 3 Complexes
- Rate: ~65-68
- Rhythm: Regular
- Axis: Normal
Intervals:
- PR – Normal (~160ms)
- QRS – Normal (100ms)
- QT – 400ms (QTc Bazette ~420-430 ms)
Segments:
- ST Depression I, II, III
Additional:
- P Wave Inversion Lead I
Interpretation:
- Ectopic Atrial Rhythm with ischaemic features
Subsequent ECG
- Ventricular ectopic with ‘R-onT’ phenomenon
- Polymorphic VT –> VF
Interpretation:
- Acute myocardial ischaemia / infarction causing polymorphic VT / VF
OUTCOME
What happened next ?
- CPR
- Received 4 x 200J shocks
- 150mg iv amiodarone
- 100 mg iv lignocaine
Subsequent ROSC was achieved after < 10 minutes. Post ROSC ECG showed anterolateral ST elevation.The patient underwent inter-hospital transfer for PCI.PCI revealed a proximal LAD lesion with 90% occlusion, which was stented.
Echo showed:
- Normal LV size with anterior, septal and apical akinesis and overall moderate systolic impairment
- Probable LV apical thrombus
- Normal right ventricular size and apical akinesis and overall mild systolic impairment.
The patient was subsequently discharged on warfarin, anti-platelet therapy, ACE inhibitor, beta-blocker, and a statin.
CLINICAL PEARLS
Things to think about
- The role of early revascularisation with thrombolysis prior to inter-hospital transfer
- The role of lignocaine/lidocaine in shock refractory VT/VF
- Several International Guidelines on ALS are linked to below and the recommendations on the use of lignocaine vary between guidelines
References
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 100 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |