
![]()
Eighth Cranial Nerve Lesions
Cranial nerve VIII is also known as the Vestibulocochlear nerve.
It conveys:
- The afferent fibres of the vestibular system
- The special sense of hearing
Lesions of CN VIII result in:
- Loss of hearing — one of the five special senses
- Debilitating disturbances in balance sensation and control
Anatomy
Course of the Vestibulocochlear Nerve
- Central nuclei:
- Vestibular nuclei → pons and rostral medulla
- Cochlear nuclei → pons and rostral medulla
- Cochlear fibres → medial geniculate bodies → superior temporal gyrus
- Vestibular fibres → widely project throughout brainstem and cerebellum
- Emerges lateral to the Facial nerve in the pontomedullary junction
- Travels through the internal acoustic meatus with CN VII and labyrinthine artery
- Terminates in the labyrinth of the inner ear (petrous temporal bone)
Vestibulocochlear Nerve Innervations
| Component | Innervations |
|---|---|
| Cochlear nerve | Special sense of hearing (organ of Corti) |
| Vestibular nerve | Sensory input from semicircular canals, utricle, saccule → essential for balance |
Pathology
Classification of Hearing Loss
| Type | Pathology |
|---|---|
| Conductive | Abnormality of external or middle ear |
| Sensorineural | Abnormality of inner ear, cochlear nerve, or brainstem |
| Mixed | Combination of conductive and sensorineural |
Causes of Cochlear Nerve Dysfunction
Sensorineural Causes
Acute
| Cause | Notes |
|---|---|
| Idiopathic Sudden Sensorineural Hearing Loss (ISSHL) | Most cases fall here |
| Noise-induced | Prolonged noise exposure |
| Meniere’s syndrome | Sensorineural loss + episodic vertigo + tinnitus |
| Ototoxic drugs | Aminoglycosides, quinine, aspirin, frusemide |
| Labyrinthitis | Viral/bacterial; associated vertigo and hearing loss |
| Acoustic neuroma | Progressive hearing loss |
| Small vessel disease | Hyperviscosity, autoimmune, microvascular |
| Brainstem lesions | Rare |
Chronic
| Cause |
|---|
| Presbyacusis (age-related loss) |
| Congenital infections (rubella, syphilis) |
Conductive Causes
Acute
| Cause |
|---|
| Wax (cerumen) impaction |
| Otitis media (acute/chronic/secretory) |
| Barotrauma |
| Temporal bone fracture |
| Tympanic membrane trauma |
| Ossicular dislocation |
| Perilymphatic fistula |
Chronic
| Cause |
|---|
| Otosclerosis |
| Paget’s disease |
Clinical Assessment
History
Key questions:
- Nature of hearing loss
- Acute / gradual
- Partial / complete
- Unilateral / bilateral
- Pain (infection, malignancy)
- Trauma (including ear cleaning)
- Noise exposure
- Middle ear symptoms
- Associated symptoms
- Tinnitus: Often accompanies nerve or conductive deafness
- Vertigo: Suggests vestibular involvement
- Medications (esp. ototoxic drugs or overdose)
Examination
| Step | Findings |
|---|---|
| Inspect external auditory meatus | Cerumen, foreign body |
| Inspect tympanic membrane | Infection, inflammation, fluid |
| Inspect for vesicles | Ramsay Hunt syndrome |
| Hearing tests | See below |
Hearing Tests
Rinne’s Test
| Step | Interpretation |
|---|---|
| 512 Hz tuning fork on mastoid → move to external meatus | AC > BC = Rinne positive (normal or sensorineural loss); BC > AC = Rinne negative (conductive loss) |
Note: Rinne alone cannot confirm sensorineural loss → requires Weber test.
Weber’s Test
| Step | Interpretation |
|---|---|
| 512 Hz tuning fork on mid-forehead | Localises to good ear = sensorineural loss; localises to bad ear = conductive loss |
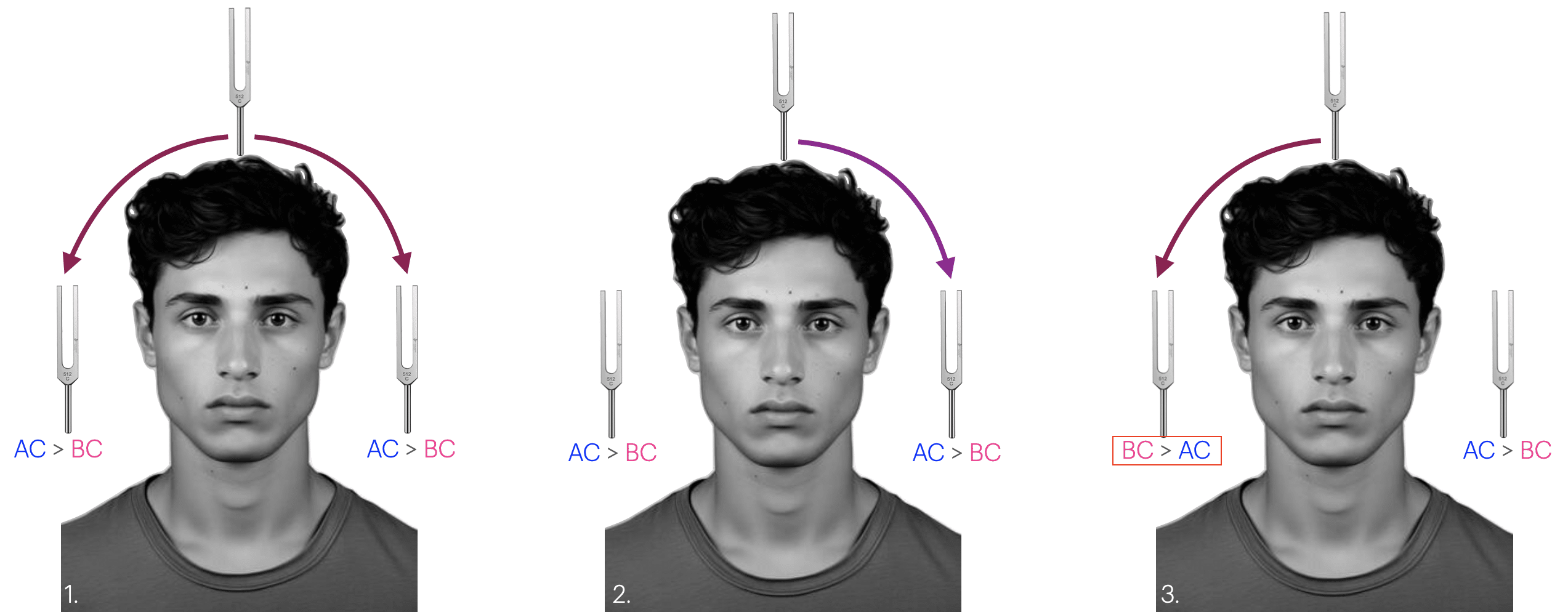
| Figure | Interpretation |
|---|---|
| 1 | Normal results: Rinne test: positive on both sides (Air conduction>Bone Conduction) Weber test: normal referred equally to each ear, indicating symmetrical hearing in both ears with normal middle/outer ear function |
| 2 | Sensorineural deafness in the RIGHT ear: Rinne test: positive on both sides Weber test: referred to the left ear. |
| 3 | Conductive deafness in the RIGHT ear: Rinne test: negative on the right (patients right) (Bone Conduction>Ait Conduction) Rinne test: positive on the left Weber test is referred to the right ear |
Audiometry
- Formal audiology assessment
- Definition of acute hearing loss:
Sensorineural loss ≥ 30 dB across ≥ 3 contiguous frequencies within 3 days
Investigations
Blood Tests
- FBC
- U&Es / glucose
- CRP
- ESR
- Others as indicated
CT Scan / CT Angiogram
- Screening for mass lesions
- CT angiogram → suspected aneurysm
MRI
- Imaging of choice
- Detects:
- Middle ear pathology
- Posterior fossa lesions
- Brainstem lesions
- Vestibulocochlear nerve pathology (e.g. acoustic neuroma)
Management
- Directed at underlying cause
- Sudden sensorineural hearing loss = otologic emergency → ENT referral prior to ED discharge
- Treat underlying causes:
- Infections → antibiotics/antivirals
- Vestibular disorders → ENT management ± vestibular rehab
- Tumours → neurosurgical or oncologic referral
- Trauma → ENT or neurosurgical management
References
Publications
- Brazis PW, Masdeu JC, Biller J. Localization in Clinical Neurology. 8e 2021
- Fuller G. Neurological Examination Made Easy. 6e 2019
- O’Brien M. Aids to the Examination of the Peripheral Nervous System. 6e 2023
FOAMed
- Cadogan M. Tuning Fork Tests (Weber and Rinne). LITFL
- Coni R. Neuro 101: Cranial Nerves. LITFL
- Nickson C. The Brainstem Rules of Four. LITFL
- Ercleve T. The rule of 4 of the brainstem. LITFL
- Nickson C. Cranial nerve lesions DDx. LITFL
Fellowship Notes

MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner

Educator, magister, munus exemplar, dicata in agro subitis medicina et discrimine cura | FFS |