
![]()
The rule of 4 of the brainstem
If you have ever wondered how a Horner’s syndrome could be associated with ipsilateral ataxia and contralateral alteration in temperature sensation? Or, why you should not be surprised to find a III nerve palsy, with a contralateral hemiparesis and loss of vibration sense? If you answered yes to these questions then you should read Peter Gates’ The Rule of 4 of the Brainstem (Int Med J 2005;263-266 – PDF).
In this beautifully written paper, Gates devises a system of approaching clinical brainstem neuroanatomy in a series of 4 simple rules. It is elegant, by explaining only that which can be detected by a basic neurological examination, and it is practical, by offering a system that can be easily remembered.
Whilst well written, the illustrations unfortunately did not reflect the simplicity of the text. Given the limitations of the images, I found myself having to rewrite the text into several tables in order to grasp the concept of the paper.
Download the full version – LITFL Rule of 4 JPG or LITFL Rule of 4 PDF
It has been quite a few years now since my exams, but I promised myself then that I would revisit the paper and try to recreate an illustration that I would like to have seen in the original publication. To this endeavor, I had to re-discover the essence of what made the paper so good, and create an illustration, which contained each of those elements.
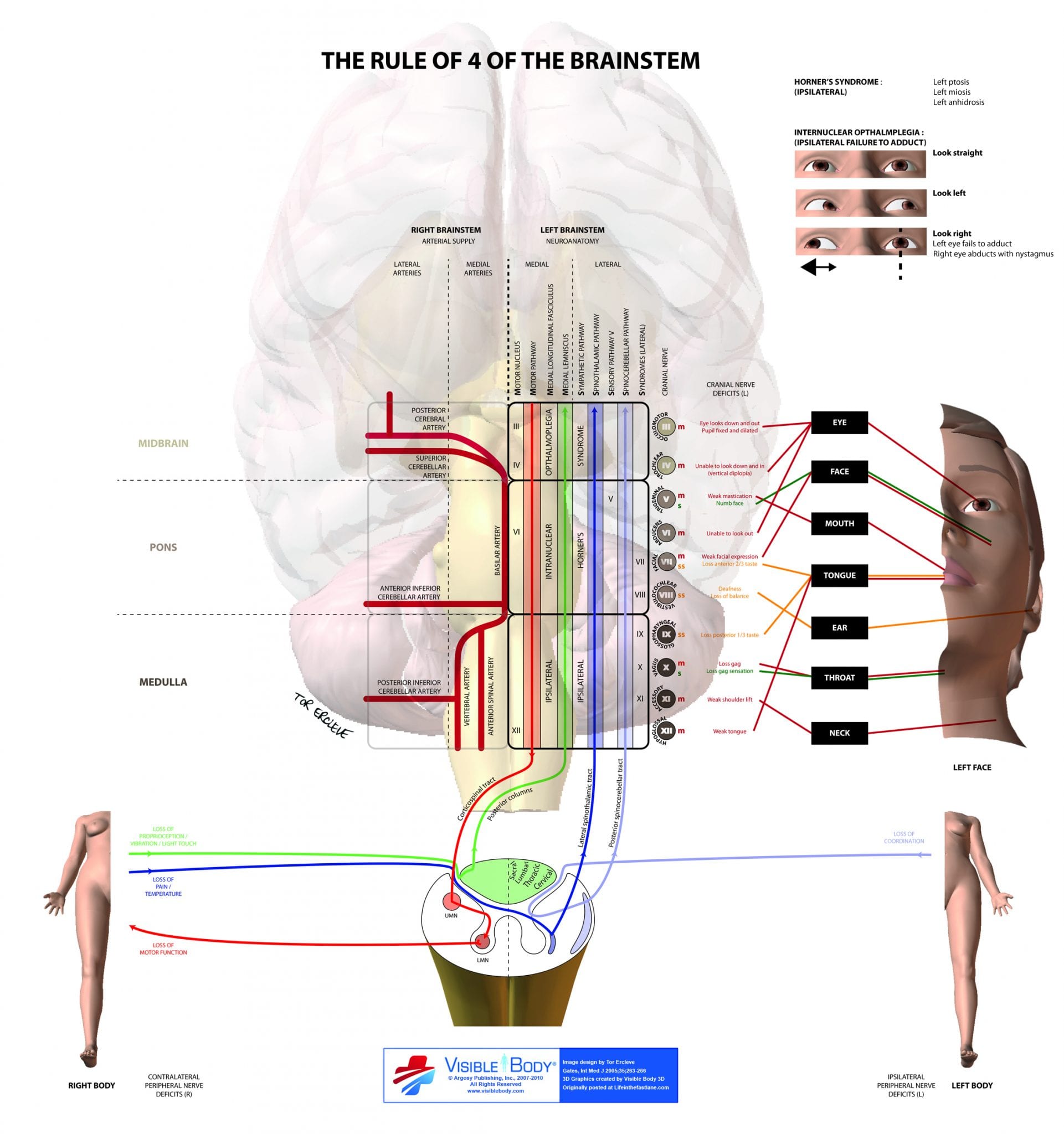
Firstly, my illustration had to include the structure of the brainstem with its 4 sets of 4 rules. They were
- There are 4 cranial nerves in the medulla, 4 in the pons and 4 above the pons
- The 4 motor nuclei that are above the nuclei that are in the midline, are those that divide equally into 12, except for I and II, that is III, IV, VI and XII. V, VII, IX and XI are in the lateral brainstem
- There are 4 columns in the ‘midline’ beginning with M.
- There are 4 columns to the ‘side’ beginning with S. (I added a fifth column to help visualize the location of the lateral 5 nerves)
Originally, I wanted to draw these lines of latitude (rules 1 and 2) and longitude (rules 3 and 4) directly onto a picture of the brainstem (see background image). Whilst this would have been more accurate, I opted rather to accentuate the principles of latitude and longitude by using a 3×9 grid. The 3 being the medulla, pons and midbrain, and the 9 being the 4 medial columns and the 4+1 lateral columns.

Next, I noticed that there were 4 columns that were in fact related to spinal tracts. Would it not be helpful to show that the medial lemniscus is the continuation of the posterior column, or that the spinothalamic pathway is in fact an extension of the lateral spinothalamic tract? Prior knowledge of spinal cord lesions would then facilitate an understanding of the brainstem pathology. It would also highlight why most clinical findings are contralateral to the cranial nerve lesion.
This leads us to the next aspect of the paper, the bringing together of form (neuroanatomy) and function (clinical findings). The illustration would have to show the clinical finding, for any given lesion on the grid. The image would have to include one side of the face and both sides of the body. For simplicity, I decided to concentrate on what you would expect to find, for a left sided brainstem lesion.

Also, there were 2 columns, one medial and one lateral, which stuck out like a sore thumb. The medial longitudinal fasciculus and the (lateral) sympathetic pathway would require a separate note (top right) to illustrate the clinic findings of a Horner’s syndrome and internuclear opthalmoplegia.
Finally, something was still missing. A clue to that component is found on the opening line of the paper: “The rule of 4 is a simple method developed to help ‘students of neurology’ to remember the anatomy of the brainstem and thus the features of the various brainstem vascular syndromes”
The rule of 4 does not just link neuroanatomical lesions to clinical signs, but also identifies the underlying vascular lesion causing them. The illustration would have to include a partial Circle of Willis divided into 6 vascular areas.
It is a known truth, that if you were to use the tube map of London to help navigate your walk from Paddington to Piccadilly Circus, you had better bring a compass, a packed lunch and camping gear. The tube map sacrifices geographical accuracy for coherent simplicity. Many more commuter hours were saved in providing a quick route planner, than there were wasted in encouraging commuters to wait for the next train from Leicester Square to Covent Garden. I hope I have done this paper justice in providing such a route planner of the brainstem. If only the London Underground could be as straightforward as clinical neuroanatomy.
Email: mike [at] litfl.com for CC license and full size image [4MB PDF]
The illustration was created using Visible Body 3D, Adobe Illustrator and Adobe Photoshop for a neurology workshop at UWA. I would like to thank Dr P Gates for making brainstem anatomy accessible to us mere mortals. Perhaps he would next like to venture into the realms of the glomerulonephritides?
References
- Gates P. The rule of 4 of the brainstem: a simplified method for understanding brainstem anatomy and brainstem vascular syndromes for the non-neurologist. Internal Medicine Journal 2005; 35: 263-266 [PMID 15836511]
- Goldberg S. Clinical Neuroanatomy Made Ridiculously Simple. MedMaster Series, 2000 Edition.
- Patten J. Neurological Differential Diagnosis. Springer-Verlag.
LITFL Links
- Brainstem Rules of 4 (original rules)
- Helpful Brainstem Figures (original figures)
- The rule of 4 of the brainstem (Rules re-imagined)
- A spider called Willis
- Using the Brainstem 1
- Using the Brainstem 2
- The Magic of the Neuro Exam
- Look Left, Look Right (Internuclear Ophthalmoplegia)
- More Befuddling Pupillary Asymmetry (Horner Syndrome)


This is excellent! Thank you for your tremendous effort in the name of FOAMed, invaluable for FEx written study
what is the green S and yellow SS in the right side of this diagram, thanks
S = sensory, and SS = special sensory.
This is genius, but I believe there is a small correction to be made. I may be wrong, but although the medial longitudinal fasciculus does join with cranial nerve nuclei in the medulla, that section of it isn’t relevant for eye movement, meaning that a lesion of the medial medulla would not produce a an internuclear ophthalmoplegia.
This is backed up by the fact that internuclear ophthalmoplegia is not mentioned in any description of medial medullary syndrome (AKA Dejerine syndrome) that I’ve been able to find, apart from one paper which appears to be under the same misapprehension that I initially was.
I would be grateful for anyone else’s thoughts.