
![]()
Femoral nerve lesions
Femoral nerve injury causes leg extension weakness, impaired hip flexion, and sensory loss over the anterior thigh and medial leg. Often traumatic in origin
Femoral nerve lesions are characterized predominantly by:
- Paralysis of the quadriceps, leading to failure of leg extension and some weakness of hip flexion
- Variable sensory loss over the antero-medial thigh, anterior knee, medial lower leg, and medial foot to the base of the great toe
Anatomy
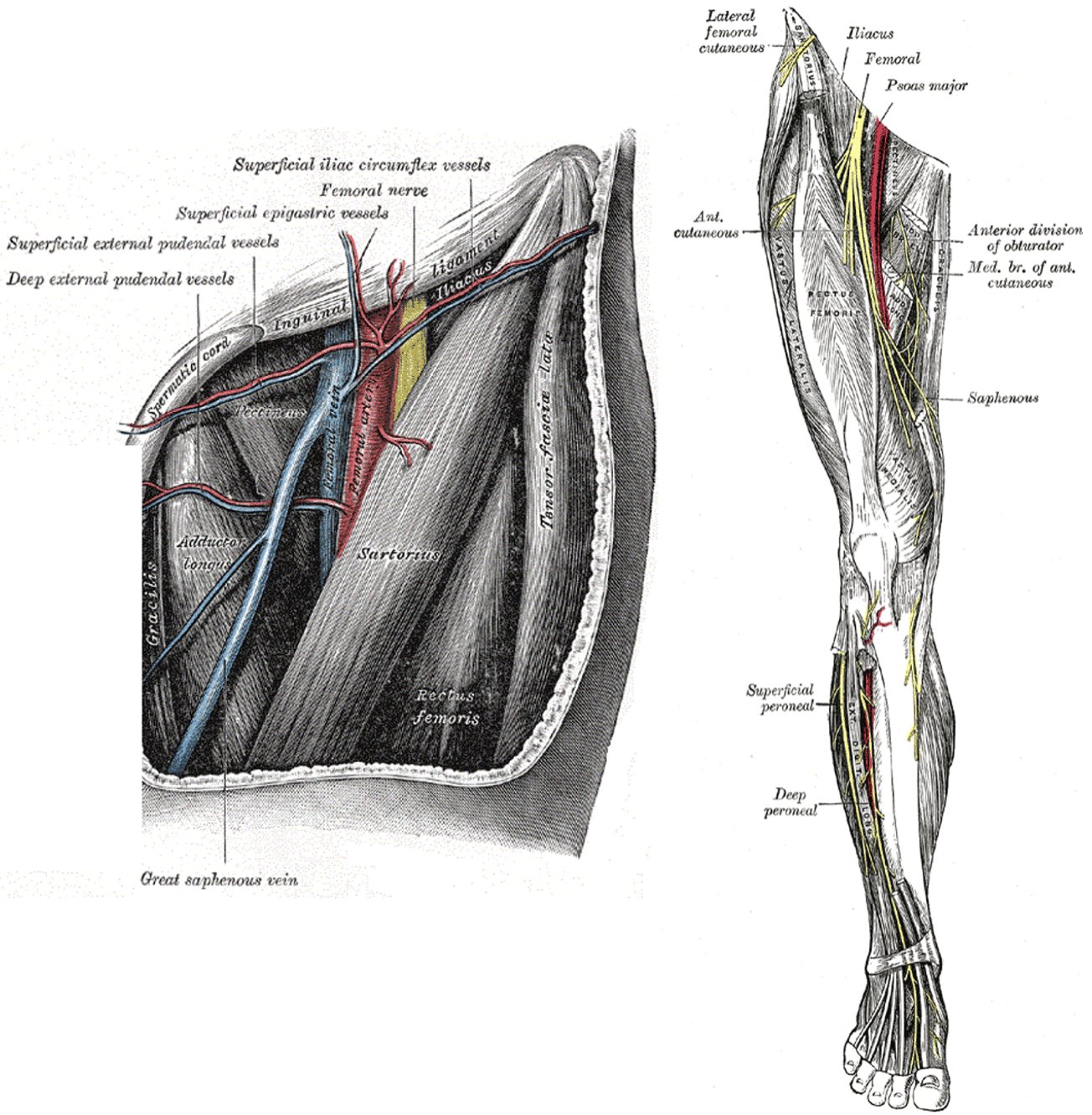
Course of the femoral nerve
- Originates from L2, L3, L4 via the lumbar plexus
- Emerges lateral to psoas, passes beneath the inguinal ligament
- Enters femoral triangle lateral to femoral artery
- Divides ~5 cm below ligament into:
- Anterior division
- Posterior division, which continues as the saphenous nerve
- Descends through adductor canal
- Emerges between sartorius and gracilis
- Runs with saphenous vein, anterior to medial malleolus to the medial foot
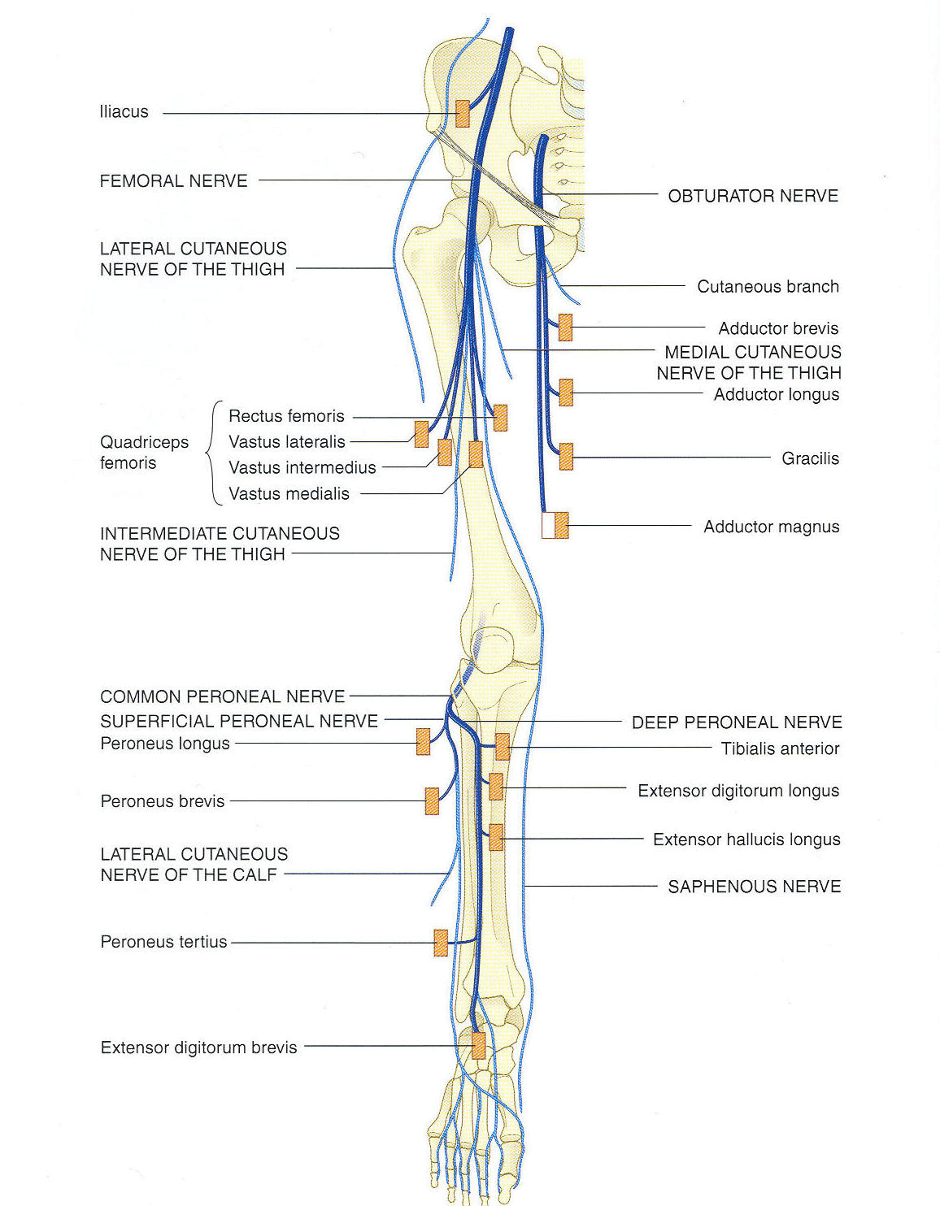
Femoral nerve innervations
Anterior division:
- Medial femoral cutaneous nerve (medial thigh)
- Intermediate femoral cutaneous nerve (anterior thigh)
- Nerve to sartorius
- Nerve to pectineus
Posterior division:
- Saphenous nerve (medial leg/foot to great toe base)
- Muscular branch to quadriceps femoris
PathologyCauses of femoral nerve lesions
- Trauma:
- Direct blunt or penetrating injury
- Especially within the femoral triangle (superficial course)
- Associated with femoral shaft fractures
- Neuropraxia:
- e.g., due to anterior thigh compartment syndrome
- Mass lesions:
- Tumours
- Abscesses
- Aneurysms
- Neuropathies:
- Rarely affects femoral nerve in mononeuropathies
Clinical Assessment

Typical features include:
- Weak hip flexion
- Loss of knee extension
- Sensory deficits in the described cutaneous distributions
Investigations
When the diagnosis is clear, investigation may not be required.
Consider based on clinical suspicion:
Blood tests:
- FBC
- U&Es / Glucose
- CRP
- ESR
- Heavy metals or others as clinically indicated
Nerve conduction studies:
- Confirm diagnosis
- Rule out generalised neuropathy
- Determine extent and prognosis
CT / MRI:
- Assess for mass lesions or direct nerve visualization
Nerve biopsy:
- Rarely indicated
- Consider in:
- Mononeuritis
- Suspected leprosy
Management
- Treat underlying cause
- Fasciotomy for compartment syndrome if indicated
- Occupational therapy:
- Supportive devices/splints
- Physiotherapy:
- Aid recovery or prevent complications
Disposition
Dependent on:
- Cause
- Severity
- Onset timing
Appendix 1
Common Peroneal Nerve Anatomy
Appendix 2
References
Publications
- Brazis PW, Masdeu JC, Biller J. Localization in Clinical Neurology. 8e 2021
- Fuller G. Neurological Examination Made Easy. 6e 2019
- O’Brien M. Aids to the Examination of the Peripheral Nervous System. 6e 2023
FOAMed
- Coni R. Neuro 101: Peripheral Nervous System. LITFL
- Nickson C. Myotomes and Differentiating Nerve Lesions. LITFL
Fellowship Notes

MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner

Educator, magister, munus exemplar, dicata in agro subitis medicina et discrimine cura | FFS |