
![]()
Fenestrated Tracheostomy Tube
ITEM NAME
- fenestrated tracheostomy tube
USES
- allows patient to breath normally with a tracheostomy in situ
- patient can cough and speak through mouth
- improves swallow function
- acts a step prior to decannulation
DESCRIPTION
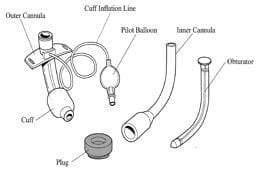
- comes with an outer cannula, inner cannula, obturator, cuff and plug
- outer cannula = keeps stoma from closing
- inner cannula = can be removed for cleaning
- obturator is used when putting the outer cannula into the stoma
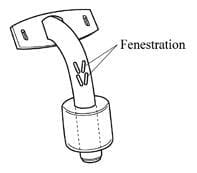
- fenestrations are holes on the posterior part of the tube above the cuff
- with the cuff up and a non-fenestrated inner cannula there is no air leak
Vocalisation
- need to remove inner cannula or use a fenestrated inner cannula
- need to occlude the outer cannula opening with a plug, speaking valve or finger
- on expiration with the cuff deflated, air passes upwards through the cords through the fenestration and around the tube enabling vocalisation
METHOD OF INSERTION
- see tracheostomy insertion techniques
What if it falls out?
- falls out and is < 5 days old -> reintubate orally
- if falls out after 5 days -> don’t worry can re-insert
OTHER INFORMATION
Complications
- suctioning without an inner cannula -> tubing going though fenestration and damaging posterior wall of trachea
- aspiration
- requirement for a surgical procedure
Immediate
- haemorrhage
- surgical emphysema
- pneumothorax
- air embolism
- cricoid cartilage damage
- pretracheal dilation and placement
- endobronchial placement
- cuff herniation
- occlusion of tip by carina or tracheal wall
- transfixation of trachea and placement in the esophagus
- …death
Delayed
- infection (tracheostomy site, larynx, tracheobronchial tree, mediastinum)
- obstruction with secretions
- ulceration/perforation (mucosal, inominate artery, tracho-oesophageal fistula)
- dysphagia c/o mechanical compression of oesophagus (requires N/G or PEG for enteral nutrition)
- problems with decannulation -> emergency airway management
Late
- tracheal granulomata
- tracheal or laryngeal stenosis
- persistent sinus @ tracheostomy site
- tracheomalacia
- aphonia/dysphonia (recovery of voice, laryngeal or cord dysfunction)
- tracheoesophageal fistula
- tracheal dilatation
References and Links
litfl.com
Social media and web resources
- UK National Tracheostomy Safety Project at www.tracheostomy.org.uk

Critical Care
Compendium
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC