
![]()
FFS: BPPV
Benign Paroxysmal Positional Vertigo (BPPV) is a common cause of vertigo, characterised by brief episodes of dizziness triggered by specific head movements. It is essential in the emergency department (ED) to differentiate BPPV from more serious central causes of vertigo
Pathophysiology
BPPV occurs when calcium carbonate crystals (otoconia) dislodge from the utricle and migrate into the semicircular canals, most commonly the posterior canal. These crystals disrupt normal fluid movement, leading to false signals about head position and causing vertigo
Causes
- Idiopathic: Most cases have no identifiable cause.
- Secondary to:
- Head trauma
- Vestibular neuronitis
- Ménière’s disease
Epidemiology
- Age: Most prevalent in individuals aged 50–70 years.
- Gender: Higher incidence in females.
- Prevalence: Increases with age; up to 9% in the elderly
Clinical Features
- Vertigo: Brief episodes (seconds to minutes) triggered by head movements such as lying down, sitting up, or rolling in bed.
- No auditory symptoms: Absence of hearing loss or tinnitus.
- Duration: Episodes typically subside over weeks.
- Dix-Hallpike Manoeuvre: Diagnostic test eliciting vertigo and nystagmus when positive .
Differential Diagnoses
- Vestibular neuronitis
- Labyrinthitis
- Ménière’s disease
- Vertebrobasilar insufficiency
- Cerebellar or brainstem stroke
- Orthostatic hypotension
Investigations
While BPPV is diagnosed clinically, further investigations may be warranted to exclude other causes:
- Imaging:
- CT Scan: To rule out central causes.
- MRI/MRA: Preferred for posterior fossa evaluation
Management
Symptomatic Treatment:
- Hydration: IV fluids for patients with significant nausea or vomiting.
- Medications:
- Prochlorperazine: For nausea and vertigo.
- Diazepam: For severe symptoms; use with caution.
- Promethazine: Alternative antiemetic.
Physical Maneuvers:
- Epley Maneuver: Repositions otoconia; first-line treatment.
- Semont Maneuver: Alternative repositioning technique.
- Brandt-Daroff Exercises: Home-based exercises for refractory cases
Disposition
Patients with unresolved symptoms may require short-term admission for further management. Physiotherapy referral for instruction on home exercises can be beneficial.
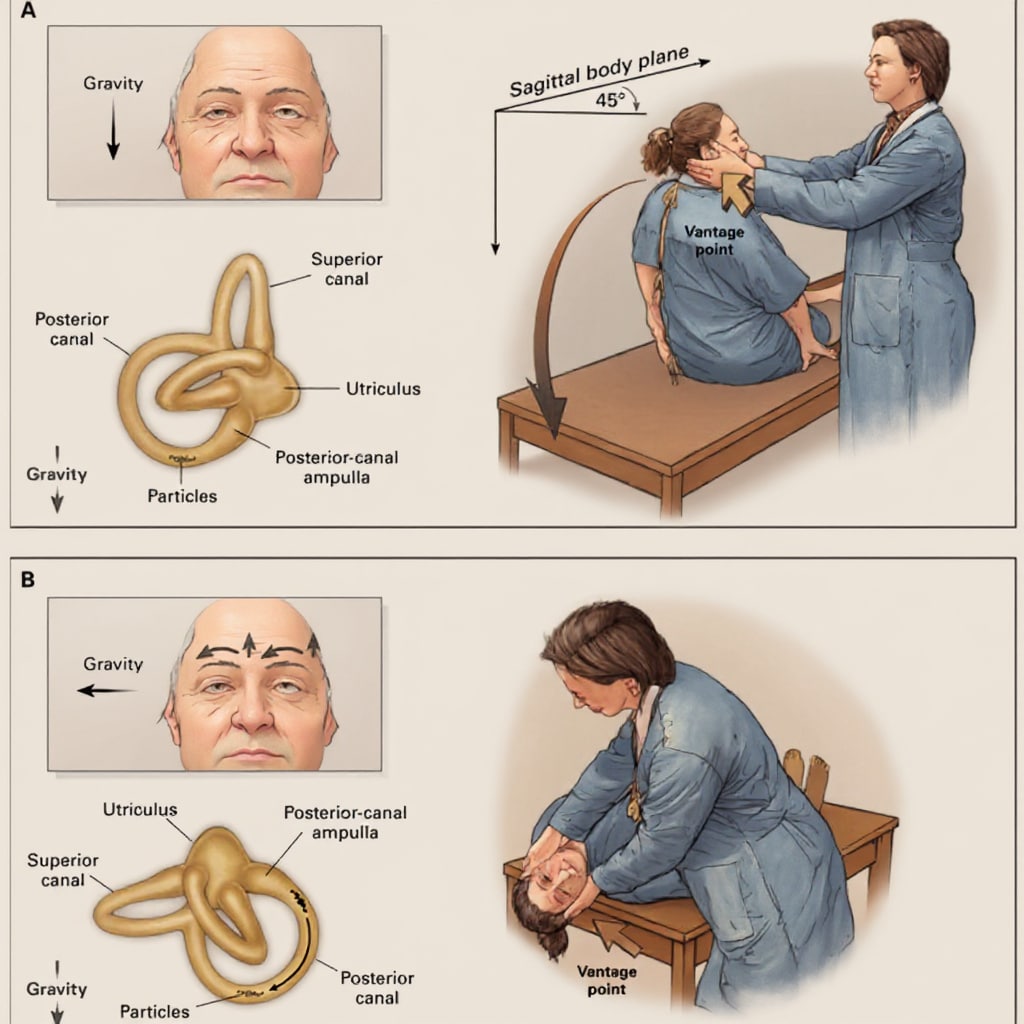
Appendix 1: Dix-Hallpike Manoeuvre
- Purpose: Diagnostic test for BPPV.
- Most expertly performed by the ED physiotherapist
- Procedure:
- Patient sits upright; head turn 45° to one side looking at examiner
- Rapidly lie the patient back with head hanging off the edge of the bed 20° extended.
- Observe for nystagmus and inquire about vertigo.
- After waiting for about 20-30 seconds, the patient is returned to the sitting position
- If no nystagmus is seen, the procedure is then repeated on the left side
Special considerations and tips
- Protect the spine (particularly the cervical spine).
- Avoid hyperextension of the neck and sudden violent movements
- Check that the patient does not have any neck injuries or other contraindications to rapid spinal movements
- Signs and symptoms usually occur when you turn the patient’s head towards the lesion, so if you suspect disease of the right ear, you may wish to start on their right side – the non-affected side
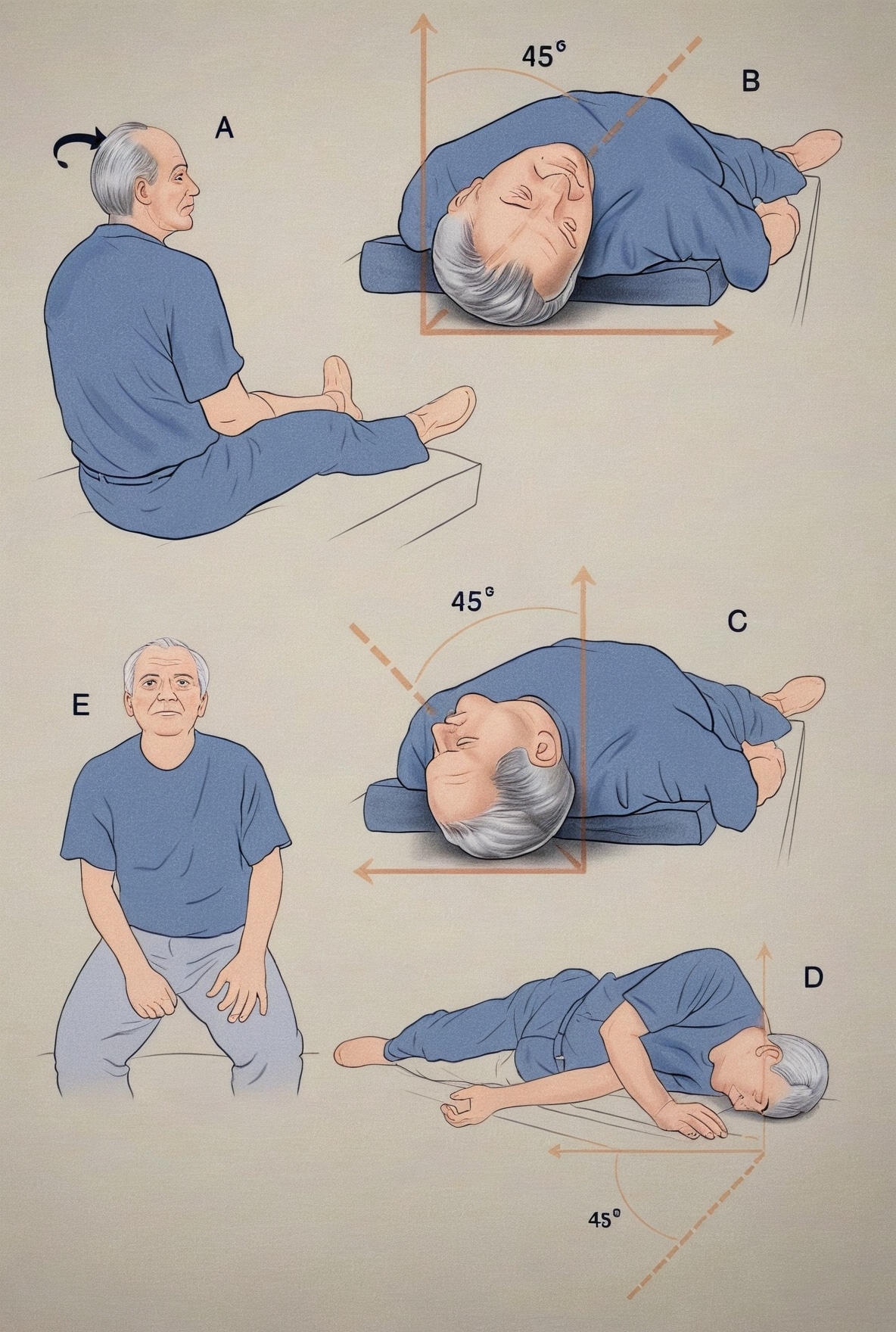
Appendix 2: Epley Manoeuvre
- Purpose: Therapeutic manoeuvre to reposition otoconia.
- Most expertly performed by the ED physiotherapist
- Procedure:
- Sequential head and body movements to guide otoconia back to the utricle.
- Typically performed by trained healthcare professionals.
- A. Position the patient on bed with head slightly extended and turned 45 degrees to the right.
- B. Position the patients with head over a pillow placed at shoulder level (as for a normal Dix-Hallpike manoeuvre) and wait one minute.
- C. Turn the head through 90 degrees and wait another minute.
- D. Turn head through a further 90 degrees, while the patient rolls on to the left side and wait another minute.
- E. Sit patient up slowly.
Appendix 3: Semont Manoeuvre
- Purpose: Alternative to the Epley maneuver.
- Most expertly performed by the ED physiotherapist
- Procedure:
- Rapid movement from lying on one side to the other to dislodge otoconia.
- The labelled boxes show the orientation of the vestibular labyrinth in each head position with the corresponding positions of the free floating deposits that eventually fall into the utricular cavity on completion of a successful particle repositioning manoeuvre
- For the treatment of right-sided disease (reverse head position for left-sided disease):
- A. Position patient on edge of bed with head turned 45 degrees to left.
- B. While maintaining this head position, tip patient to right side (also an alternative method for performing the Dix-Hallpike manoeuvre) and wait 1 minute.
- C. Move patient quickly through 180 degrees (maintaining original head position), wait another minute and then sit patient up slowly

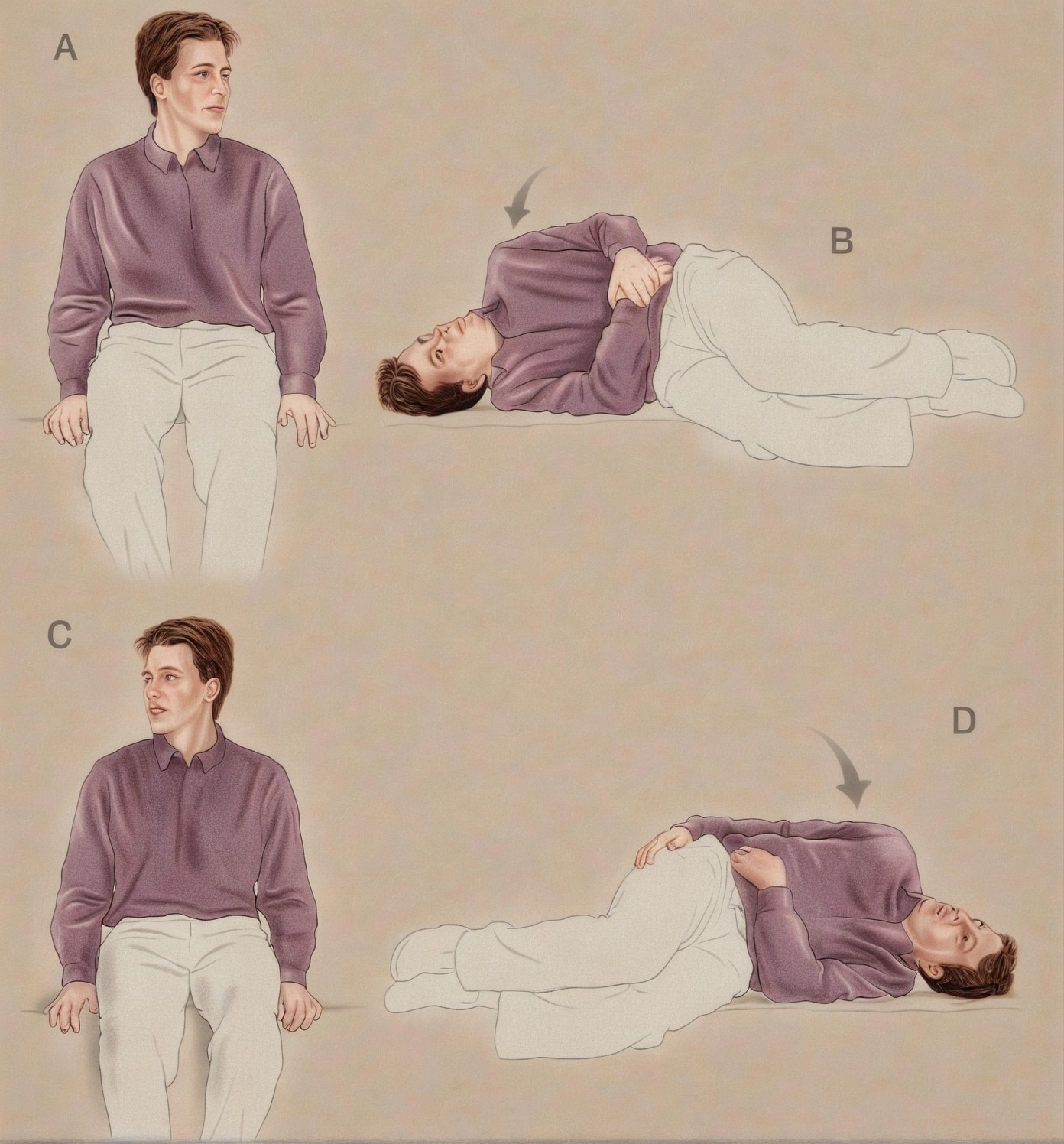
Appendix 4: Brandt-Daroff exercises
Exercises should be performed 3 times daily if possible. In the initial stages it is permissible to take an anti-sickness medication if nausea is a problem.
The symptoms of giddiness need to be reproduced by the exercises if any benefit is to occur. If the exercises are done regularly, the symptoms should resolve over a period of several days in most cases.
- A. Sit on edge of bed, turn head slightly to left side (approximately 45 degrees).
- B. While maintaining this head position, lie down quickly on the right side, so that the back of the head is resting on the bed. Wait for 20 to 30 seconds or for any giddiness to resolve.
- C. Sit up straight, again waiting for 20 to 30 seconds or for any giddiness to resolve.
- D. Turn head slightly to right side and repeat sequence in the opposite direction.
Continue as above for 10 minutes (5 or more repetitions to each side).
References
Publications
- Nelson JA, Viirre E. The clinical differentiation of cerebellar infarction from common vertigo syndromes. West J Emerg Med. 2009 Nov;10(4):273-7.
FOAMed
- Nickson C. Ballistically Potent Vertigo. LITFL
- Cassidy T. Vertigo the Big 3. LITFL
- Baker C. Benign paroxysmal positional vertigo. LITFL
- Baker C. Dix-Hallpike Test. LITFL
Fellowship Notes

MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner

Educator, magister, munus exemplar, dicata in agro subitis medicina et discrimine cura | FFS |