
![]()
Fifth Cranial Nerve Lesions
Cranial nerve V is also known as the Trigeminal nerve.
It is the largest and most complex cranial nerve
(although the vagus is the longest).
The trigeminal nerve supplies
- Sensory innervation to:
- Face
- Teeth
- Nasal cavity
- Motor supply to:
- Muscles of mastication
- Tensor veli palatini
- Tensor tympani
The commonest lesions of the trigeminal nerve include:
- Herpes zoster infection
- Multiple sclerosis (MS)
- Trigeminal neuralgia
Other lesions of the trigeminal nerve are relatively uncommon.
Variable facial numbness may be seen with presentations of MS.
Anatomy
Course of the Trigeminal Nerve
- Motor origin: Trigeminal motor nucleus, pons
- Sensory nuclei: Trigeminal sensory nucleus (pons and extends through brainstem)
- Emerges from the ventral pons via:
- Large sensory root
- Smaller motor root
- Enters middle cranial fossa
- Sensory root forms trigeminal (Gasserian) ganglion at apex of petrous temporal bone
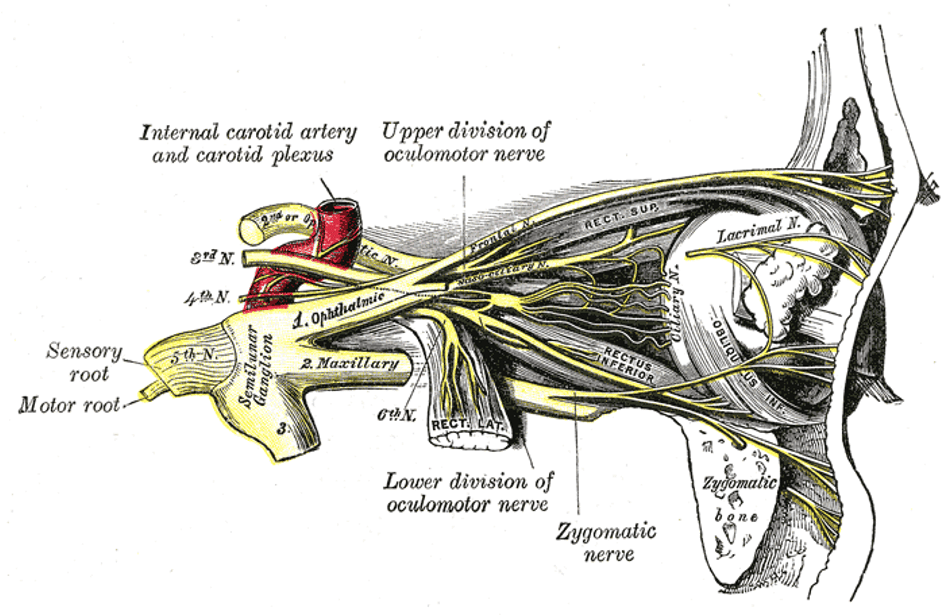
- From this ganglion arise 3 major branches:
| Branch | Foramina | Innervation type |
|---|---|---|
| Ophthalmic | Superior orbital fissure | Sensory only |
| Maxillary | Foramen rotundum | Sensory only |
| Mandibular | Foramen ovale | Sensory + Motor |
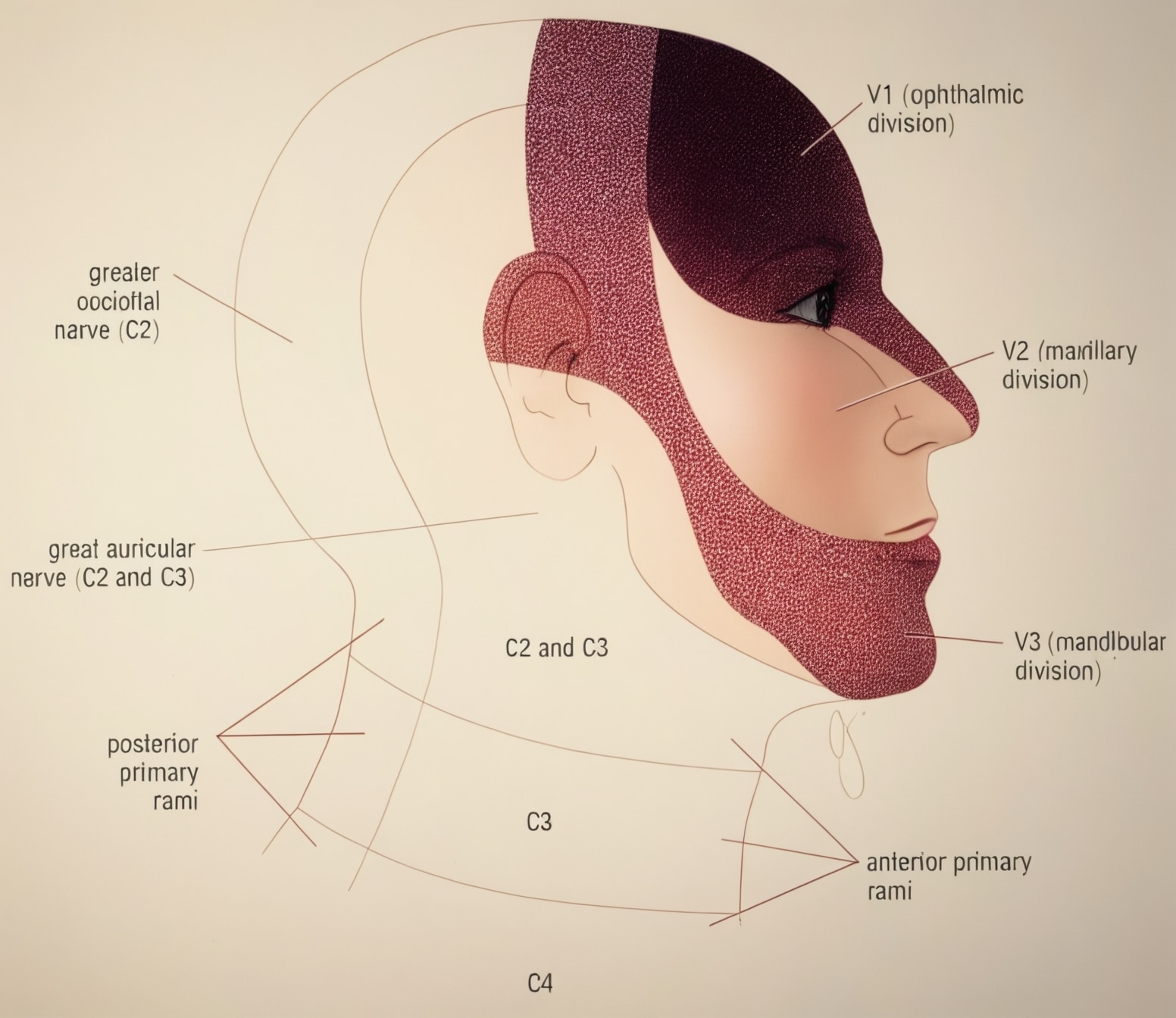
Trigeminal Nerve Innervations
1. Ophthalmic Branch (V1)
| Branch | Supplies |
|---|---|
| Lacrimal nerve | Upper lateral eyelid (sensory), parasympathetic fibres pass to lacrimal gland |
| Nasociliary nerve | Ciliary ganglion, long ciliary nerve, posterior & anterior ethmoidal nerves, infratrochlear nerve |
| Frontal nerve | Supratrochlear & supraorbital nerves |
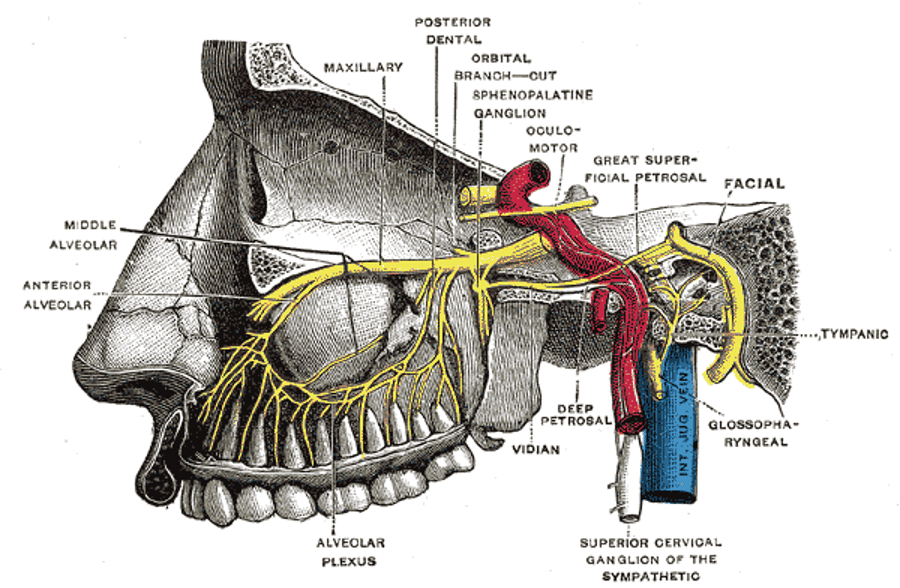
2. Maxillary Branch (V2)
| Branch | Supplies |
|---|---|
| Meningeal branches | Middle cranial fossa |
| Pterygopalatine ganglion branches | Lacrimal gland, palate, nasal cavity |
| Posterior superior alveolar nerve | Maxillary molars |
| Zygomatic nerve → zygomaticotemporal & zygomaticofacial | Lateral face, parasympathetics to lacrimal gland |
| Middle & anterior superior alveolar nerves | Maxillary teeth |
| Infraorbital nerve | Lower eyelid, cheek, upper lip |
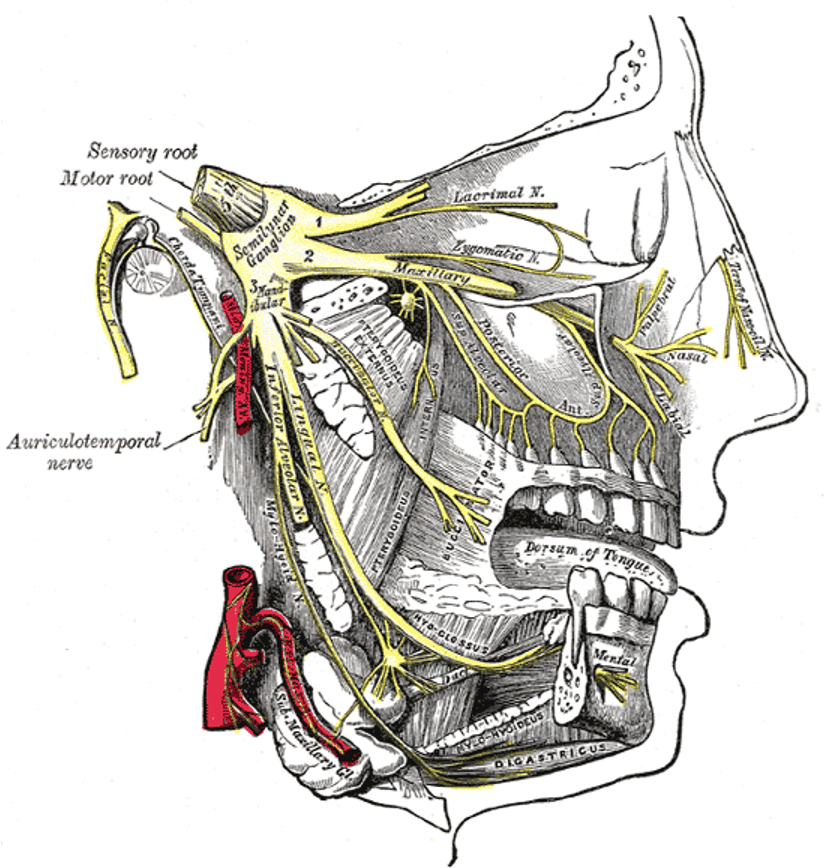
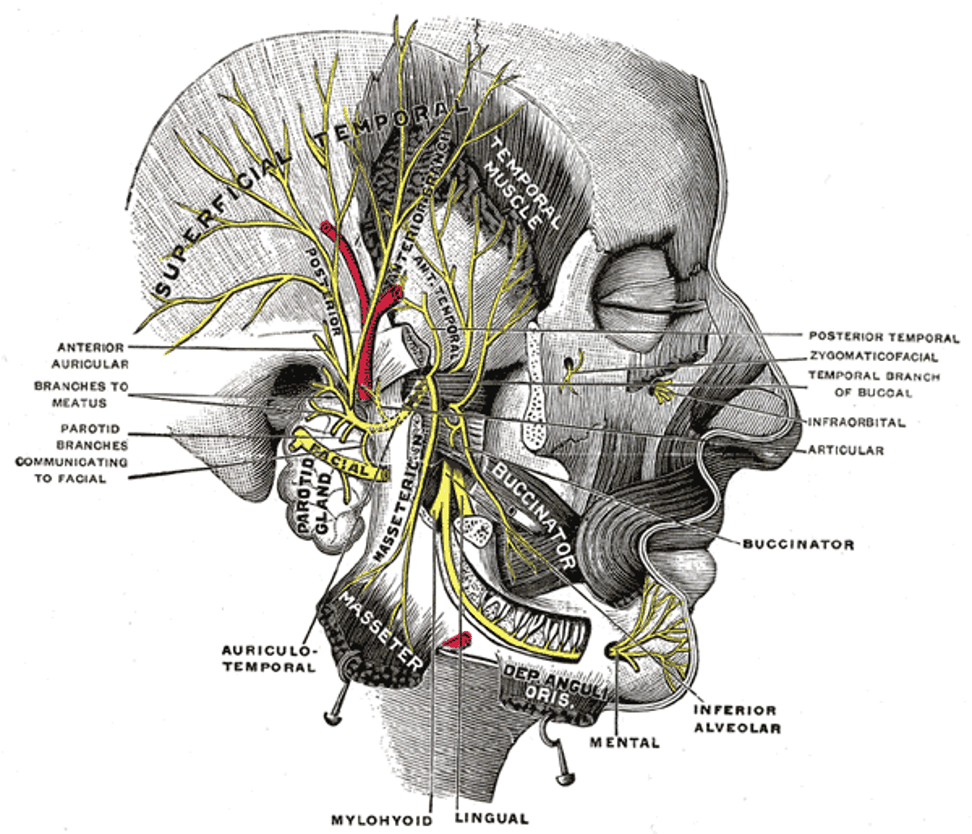
3. Mandibular Branch (V3)
| Branch | Supplies |
|---|---|
| Meningeal branch | Dura mater |
| Nerve to medial pterygoid | Medial pterygoid, tensor veli palatini, tensor tympani |
| Nerve to masseter, temporalis, lateral pterygoid | Muscles of mastication |
| Buccal nerve | Cheek mucosa (sensory) |
| Auriculotemporal nerve | Auricle, outer tympanic membrane, temporal region, TMJ, carries parasympathetics to parotid |
| Lingual nerve | Anterior 2/3 tongue (general sensation), floor of mouth; taste via chorda tympani |
| Inferior alveolar nerve → nerve to mylohyoid, mental nerve | Lower teeth, mylohyoid, anterior digastric, chin skin |
Pathology
Central Lesions
| Cause |
|---|
| Vascular lesions |
| Tumours |
| Demyelination (MS) |
| Syringobulbia |
Peripheral Lesions
| Cause |
|---|
| Space-occupying lesions (tumours, aneurysms) in middle cranial fossa |
| Cavernous sinus lesions (thrombosis, tumour, aneurysm) → can involve CN III, IV, VI |
| Skull base trauma (middle cranial fossa fractures) |
| Mononeuritis (rare) → diabetes, connective tissue disease, alcohol, paraneoplastic, sarcoidosis, HIV |
Clinical Assessment
1. Corneal Reflex
- Stimulus: Cotton bud to cornea
- Normal: Bilateral blinking
- Afferent limb: Ophthalmic branch of CN V
- Efferent limb: Facial nerve (CN VII) → orbicularis oculi
| Finding | Indicates |
|---|---|
| No blink, no sensation | Ophthalmic nerve lesion |
| Blink in contralateral eye only | Ipsilateral facial nerve palsy |
2. Facial Sensation
- Test each division (V1, V2, V3)
- Compare sides
- Pain: sterile needle or blunt stick
- Light touch: cotton wool
- Temperature: if syringobulbia suspected
3. Motor Function
- Inspect for temporal/masseter wasting
- Clench teeth → palpate masseters
- Open mouth against resistance → pterygoid function
- Jaw deviates to weak side if V3 lesion
4. Jaw Jerk Reflex
- Mouth slightly open → tap examiner’s finger on symphysis menti
- Normal: slight closure or no response
- Hyperactive: UMN lesion (e.g. pseudobulbar palsy)
Summary of Clinical Patterns
| Pattern | Likely lesion site |
|---|---|
| Loss of all 3 divisions | Central lesion or trigeminal ganglion |
| Loss of single division | Peripheral lesion post-ganglion |
| Dissociated pain/touch loss | Brainstem or cervical cord lesion |
Investigations
Blood Tests
- FBC
- U&Es / glucose
- CRP
- ESR
CT Scan / CT Angiogram
- Screening for intracranial mass lesions
- CT angiogram → suspected aneurysm
MRI
- Best modality for trigeminal nerve lesions
- Intracranial / intraorbital pathology
- Demyelination (MS)
- Tumours
- Brainstem lesions
Management
- Directed at the underlying cause
- Tumour → Neurosurgery
- MS → Neurology
- Neuralgia → Medical therapy
- Infection → ID / Neurology
- Trauma → Neurosurgery
Appendix 1
Appendix 2
References
Publications
- Brazis PW, Masdeu JC, Biller J. Localization in Clinical Neurology. 8e 2021
- Fuller G. Neurological Examination Made Easy. 6e 2019
- O’Brien M. Aids to the Examination of the Peripheral Nervous System. 6e 2023
FOAMed
- Coni R. Neuro 101: Cranial Nerves. LITFL
- Nickson C. The Brainstem Rules of Four. LITFL
- Ercleve T. The rule of 4 of the brainstem. LITFL
- Nickson C. Third Cranial Nerve Lesions. LITFL
- Nickson C. Cranial nerve lesions DDx. LITFL
Fellowship Notes

MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner

Educator, magister, munus exemplar, dicata in agro subitis medicina et discrimine cura | FFS |