
![]()
Frederic Cotton

Frederic Jay Cotton (1869-1939) was an American Orthopedic Surgeon.
Eponymously affiliated with the Cotton fracture (trimalleolar fracture) and Cotton-Loader postion (extreme palmar flexion and ulnar deviation in closed reduction of distal radius fractures)
Cotton contributed extensively to the literature on fractures and dislocations. He collaborated on ‘Treatise on Orthopedic Surgery‘ (Bradford EHH, Lovett RW.) and ‘The treatment of fractures‘ (Scudder CL) prior to publication of his own tome ‘Dislocations and Joint Fractures‘ in 1910
Biography
- Born on September 24, 1869 in Prescott, Wisconsin
- 1871 – family moved to Newport when his father took charge of the construction of the Block Island breakwater
- 1890 – Graduated Harvard College
- 1894 – AM MD, Harvard Medical School
- 1894-1897 studied bacteriology in New York, Vienna. Established the laboratory of bacteriology at the Infants Hospital
- 1898 – Surgeon in the Spanish–American War
- 1902-1932 Surgeon to outpatients at the City Hospital
- 1917 – WW I, Major in the United States Army
- Professor of surgery at Tufts College Medical School, Boston
- Died on April 14, 1938 in Boston
Medical Eponyms
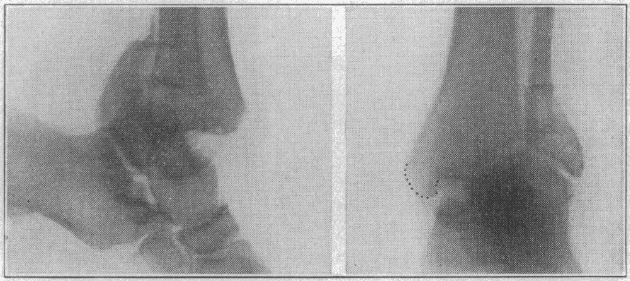
Cotton fracture (1915)
The Cotton fracture is a fracture of the ankle involving the lateral malleolus, medial malleolus and distal posterior aspect of the tibia (posterior malleolus). [aka *trimalleolar fracture ]
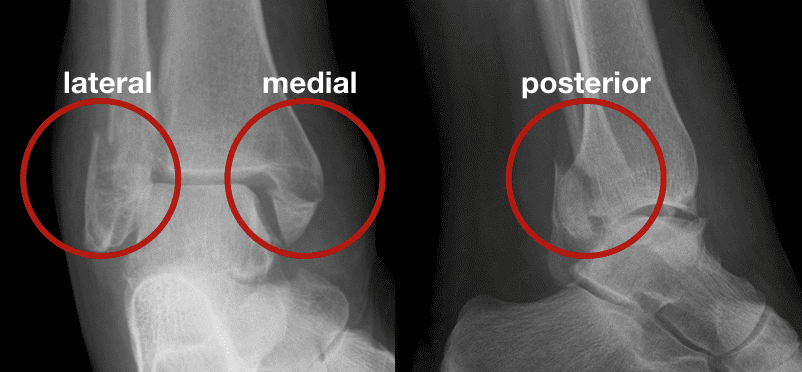
I have been talking about the lesion for years, until some of my house-officers at the City Hospital, wearied by long insistence, have come to refer to it as “Cotton’s fracture.”
The characteristic point of the fracture under consideration is backward dislocation with the splitting away of a wedge large or small from the back surface of the tibia at the joint – a wedge that is displaced backward with backward dislocation of the foot. This wedge carries the posterior tibio-astragaloid ligaments; foot and tibial fragment move together, up and backward…the posterior tibial fragment is separate, though associated with fracture of both malleoli.
Cotton 1915
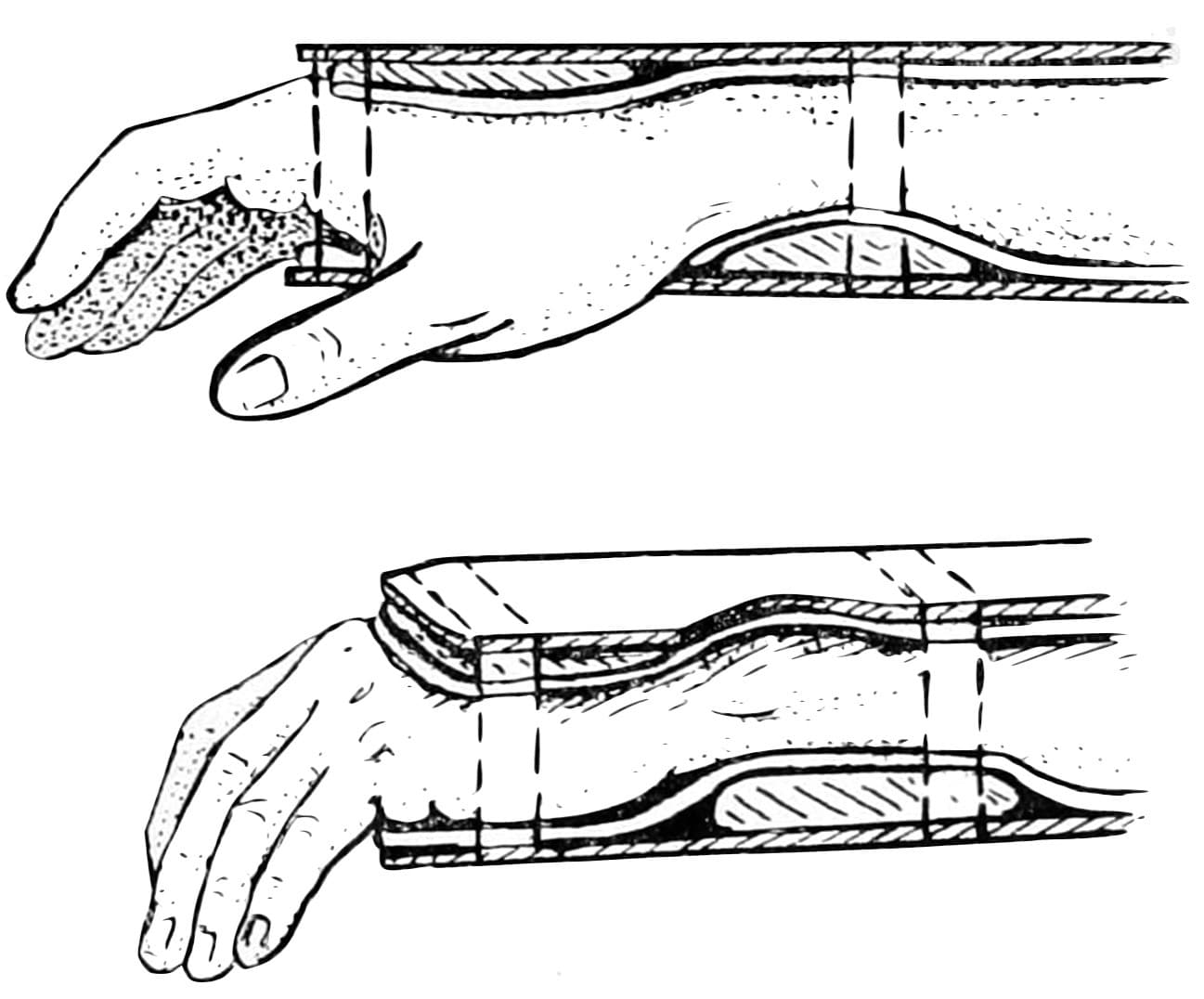
Cotton-Loder position
Extreme palmar flexion and ulnar deviation in closed reduction of distal radius fractures. Named in conjunction with his Massachusetts General Hospital surgical colleague Halsey Beach Loder (1883-1966)**
Cotton wrote extensively on the subject of fractures of the distal end of the radius, methods of reduction and treatment with appropriate padding and support.
Carpal tunnel syndrome associated with the Colles fracture was given little attention and initially felt to be a rare sequela. However, the combination of two extreme positions exposes the median nerve to a clamp and thereby to further problems.
In 1933, Abbott and Saunders identified median nerve compression as being not as rare as initially thought. It was not until this review that the popular Cotton-Loder position for immobilization of distal radius fractures was called into doubt.
In 1950, Sir John Charnley advocated the use of a modified or moderate ‘Cotton–Loder’ position to avoid extreme positions and median nerve compromise. He recommended mild flexion at the wrist with ulnar deviation. The particular casting guide described by Charnley has been preserved to this day as the most widely-used casting position in the treatment of wrist fractures.
**Halsey Beach Loder (1883-1966)
Very little biographical data is available for Dr Loder, and the specific publication conjoining his name with that of Cotton has yet to be retrieved.
Loder, Halsey B. M.D. Dartmouth Medical School 1908; F.A.C.S., Visiting Surgeon, Boston City Hospital; Consulting Surgeon, Choate Memorial Hospital, Woburn, Leonard Morse Hospital, Natick, and Nashua Memorial Hospital, Nashua.
- Loder HB. The more efficient treatment of Colles’ fractures. Boston City Hospital Alumni. 1916
- A Hint To Scientists. Boston Med Surg J 1927; 197:319-320
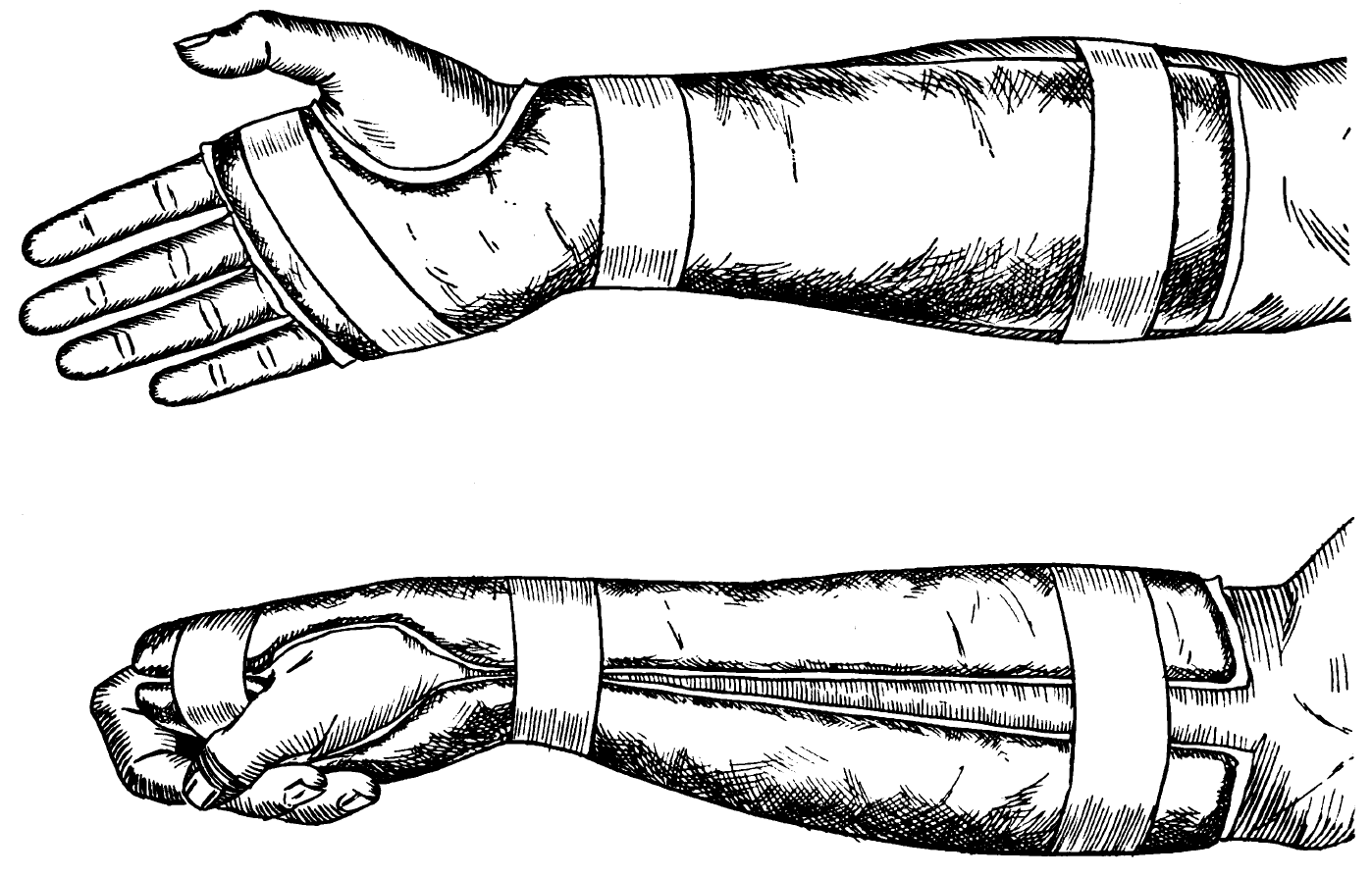
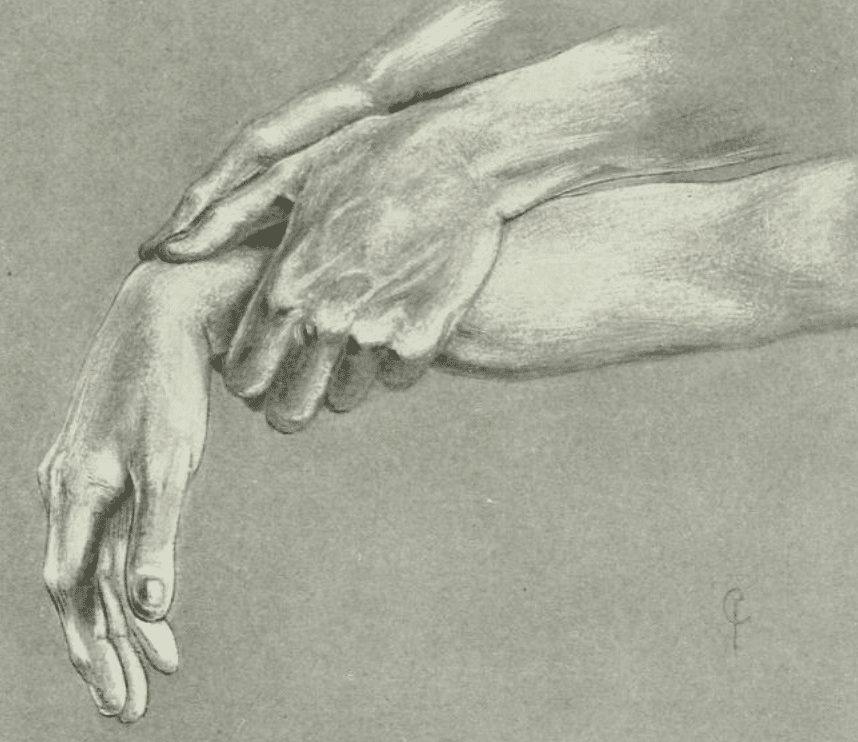
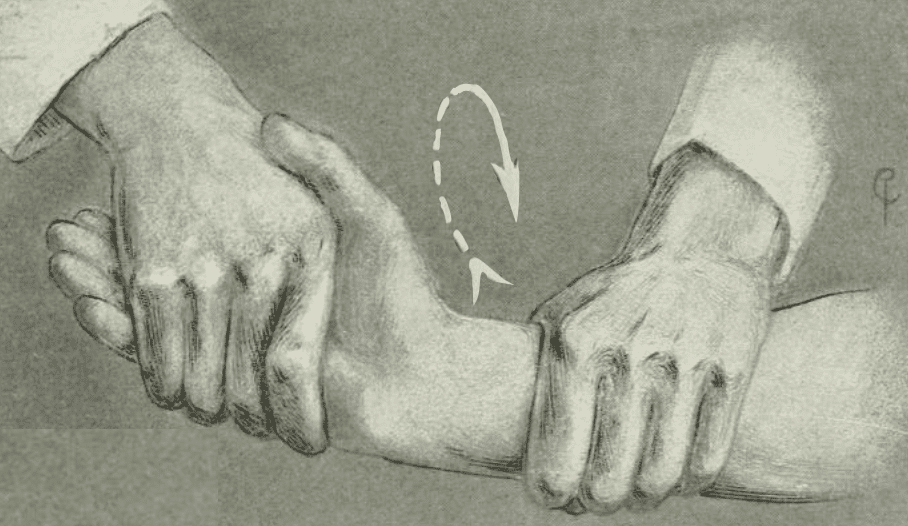
Cotton grip (1910)
Cotton provided an illustrated series of grips to manage the reduction of a Colles fracture
An assistant gives countertraction at the elbow or axilla. The surgeon may use any of the grips illustrated. The choice depends somewhat upon the amount of swelling present and the ease with which the fragment can be clasped, somewhat upon the size of the patient’s hand in proportion to the surgeon’s. More than all it depends upon the habit and convenience of the surgeon.
The writer’s usual routine is as follows: Grip 1 is used, with strong traction to start the loosening of the fragments; then Grip 3, until any impaction present is entirely loosened. Grip 6 is assumed, and circumduction of the hand in both directions is carried out, in order to untangle the possibly entangled ulna,* then the hand is brought over into sharp flexion, with a shove on the back (Grip 2), and, finally, the displacement as a whole having been reduced by these means, the hand is sharply flexed in order to make sure that the backward rotation has been overcome. Grip 4 and grip 5 give more power in reduction when this is needed.
If these manoeuvers have been carried out properly, there should be little tendency to any recurrence of deformity
Cotton 1910: 347-352




Major Publications
- Cotton FJ. Malaria as seen at Montauk. 1898
- Cotton FJ. III. The Pathology of Fracture of the Lower Extremity of the Radius. Ann Surg. 1900 Aug;32(2):194-218
- Cotton FJ. V. Elbow Fractures in Children. Fractures of the Lower End of the Humerus; Lesions and End Results, and their Bearing upon Treatment. Ann Surg. 1902 Feb;35(2):242-69
- Cotton FJ. VIII. The Pathology of Fracture of the Lower Extremity of the Radius. Ann Surg. 1900 Sep;32(3):388-415
- Cotton FJ. IX. Elbow Fractures in Children. Fractures of the Lower End of the Humerus; Lesions and End Results, and their Bearing upon Treatment. Ann Surg. 1902 Mar;35(3):365-99
- Scudder CL, Cotton FJ. The treatment of fractures, 3e 1902
- Cotton FJ. Dislocations and Joint-Fractures. W.B. Saunders. 1910 [Cotton-Loder position p353][Cotton fracture p539]
- Cotton FJ, Brickley WJ. Luxation of the ulna forward at the wrist (without fracture). Ann Surg. 1912; 55(3): 368–374.
- Cotton FJ, Boothby WM. A Warning in Regard to Intratracheal Insufflation Anesthesia; The Necessity of a Safety Valve. Boston Medical and Surgical Journal 1912; 166(13): 486
- Cotton FJ, Loder HB. The fate of bone grafts. Surgery Gynecology And Obstetrics 1913: 17: 701-703
- Cotton FJ. Hip fractures and their treatment. Boston Med Surg J 1914; 170:718-723
- Cotton FJ. A new type of ankle fracture. JAMA. 1915; 64: 318–321. [Cotton fracture]
- Cotton FJ. Adequate Reduction and Care in Colles’s Fracture; New Methods. Boston Med Surg J 1919; 181: 651-656
References
Biography
- Lund, FB. Memoir: Frederic Jay Cotton 1869-1938. Ann Surg. 1939 Feb;109(2):317-9
- Mostofi SB. Who’s Who in Orthopedics. Springer 2005: 80-81
- Personal communication with Frederic C. Chalfant
Eponymous terms
- Abbott LC, Saunders JB. Injuries of the median nerve in fractures of the lower end of the radius. Surgery, Gynecology & Obstetrics 1933; 57: 507–516
- Cadogan M. Eponymous ankle and talus injuries. LITFL
- Cadogan M. Cotton fracture. Eponym A Day. Instagram
Eponym
the person behind the name

RN, Sir Charles Gairdner Hospital. Coronary Care Unit / Emergency Department. Keen interest in critical and pre hospital care.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |