
![]()
Georges Dieulafoy
Georges-Paul Dieulafoy (1839-1911) was a French physician.
Dieulafoy was a French internist, widely admired for his diagnostic acumen and clinical teaching. Regarded as one of the great Parisian physicians of the late 19th century, he worked to bridge the traditional divide between internal medicine and surgery, and is often credited as a founding figure of modern gastroenterology.
Dieulafoy advanced the use of clinical pathology at the bedside, combining careful physical examination with pathological reasoning. His studies of pleural effusion and empyema led to the refinement of thoracocentesis and invention of the Dieulafoy aspirator (1869), a subcutaneous vacuum device for diagnosis and treatment of fluid collections.
He made significant contributions to the understanding of acute appendicitis, describing Dieulafoy’s triad (cutaneous hyperesthesia, tenderness, and muscular guarding at McBurney’s point) as an early clinical sign. At a time when appendicitis was frequently misdiagnosed or treated conservatively, Dieulafoy argued strongly for early surgical intervention, influencing a shift in Parisian surgical practice by the 1890s.
Eponymously remembered for Dieulafoy’s lesion (exulceratio simplex, 1898), a life-threatening cause of massive gastrointestinal haemorrhage, as well as a second Dieulafoy triad of hysterical blindness. His legacy lies in the union of careful clinical observation with innovative, practical therapeutics.
Biographical Timeline
- Born on November 18, 1839 – Toulouse, France
- 1863 – Moved to Paris during his third year of medical studies at Toulouse; joined the clinical department of Armand Trousseau (1801-1867) in Hôtel-Dieu
- 1865 – Placed first in the Paris hospital internship exam; became interne des hôpitaux.
- 1869 – Received his medical doctorate with a thesis titled De la mort subite dans la fièvre typhoïde. Also perfected thoracentesis and invented Dieulafoy’s aspirator.
- 1870 – Served in the Franco-Prussian War, leading an ambulance service at the Holy Trinity Church of Paris.
- 1872 – Married his cousin, Claire Bessaignet (no children). Published De la contagion and Du diagnostic et du traitement des épanchements aigus et chroniques de la plèvre par aspiration.
- 1873 – Published Traité de l’aspiration des liquides morbides.
- 1875 – Became agrégé (assistant professor) with a second thesis, Des progrès réalisés par la physiologie expérimentale dans la connaissance des maladies du système nerveux.
- 1876 – Appointed Médecin des hôpitaux (Physician of Paris Hospitals).
- 1879 – Became head of service at Tenon Hospital.
- 1880–1884 – Published Manuel de pathologie interne, a seminal textbook which saw 16 editions by 1911 and was translated into multiple languages.
- 1881 – Appointed head of service at Saint-Antoine Hospital.
- 1886 – Appointed to the chair of internal pathology at Necker Hospital.
- 1887 – Named Professor of Internal Pathology, succeeding Alfred Hardy (1811–1893).
- 1896 – Appointed Professor of Clinical Medicine at Hôtel-Dieu, succeeding Germain Sée (1818–1896).
- 1898 – First described “exulceratio simplex” (Dieulafoy’s lesion), theorizing it as an early stage of gastric ulcer interrupted by hemorrhage.
- 1899–1910 – Published Clinique médicale de l’Hôtel-Dieu de Paris in several volumes.
- 1909 – Retired from Hôtel-Dieu; became chief physician at the Léon Bourgeois Dispensary, Hospital Laennec.
- 1910 – Elected president of the French Academy of Medicine.
- Died August 16, 1911 in Paris following postoperative complications; buried at Montmartre Cemetery.
Medical Eponyms
Dieulafoy lesion (1898)
Rare but important cause of acute, often massive gastrointestinal haemorrhage. Characterised by a tiny mucosal defect overlying a disproportionately large-calibre submucosal arteriole, most commonly located on the lesser curvature of the stomach within 6 cm of the gastroesophageal junction. Accounts for 1–2% of all GI bleeds.
1876 – Théophile Jean Gallard (1828-1887) presents two cases of sudden fatal gastric haemorrhage due to “de petits anévrysmes miliaires” of the stomach at the Association Française pour l’Avancement des Sciences in Clermont-Ferrand.
1884 – Gallard publishes a further three cases in Anéurismes miliaires de l’estomac, concluding “…very small aneurysms of the stomach arteries… were the starting point for rapidly fatal haemorrhages.” – Gallard 1884
1898 – Dieulafoy coins the term exulceratio simplex and provides the first comprehensive clinicopathological description. He described cases of sudden, fatal haematemesis due to minute ulcers eroding large submucosal vessels at the gastric cardia and fundus. He emphasised that these lesions were distinct from ordinary peptic ulcers and could bleed massively without warning.
Original
English
…ces petites ulcérations, à peine visibles, peuvent déterminer des hémorragies foudroyantes et mortelles…- Dieulafoy 1898
…these small, scarcely visible ulcers can cause sudden and fatal haemorrhages…- Dieulafoy 1898
Histological specimen from Exulceratio simplex: Leçons 1–3, Clinique médicale de l’Hôtel-Dieu de Paris. 1898. The figure legend captures the critical point: the mucosal defect is tiny, but it overlies a disproportionately large submucosal arteriole, rupture of which produces “hémorragies mortelles.”

Dieulafoy recommended surgical excision as the therapeutic approach to these lesions and this remained until the introduction of endoscopy. The use of endoscopy caused prognosis to drop to 8% from 80%.
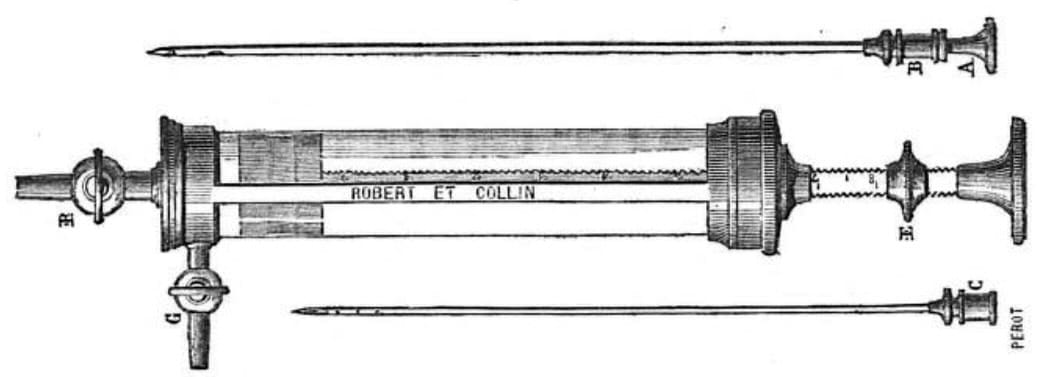
Dieulafoy aspirator (1869)
Pneumatic subcutaneous aspirator designed for diagnostic and therapeutic evacuation of deep fluid collections via controlled suction.
Comprised of a syringe chamber with a lateral valve, detachable needles and cannulae, the device allowed controlled aspiration of fluid with reduced pain and infection risk. The device was used to manage pleural effusions, synovial fluid collections, abscesses, and for suprapubic bladder aspiration, the aspirator offered a less invasive alternative to trocar puncture.
1856 – Pneumatic aspiration with un nouveau trocart aspirateur first described by Belgian physician Edouard van den Corput (1821-1908).
1869 – Dieulafoy develops a refined apparatus and technique for subcutaneous aspiration. The device was presented to the Académie de médecine on November 2, 1869 by Professor Adolphe Gubler (1821–1879) on Dieulafoy’s behalf as Un aspirateur sous-cutané destiné au diagnostic et au traitement des collections liquides profondes. The aspirator included a piston-driven syringe with lateral valve, trocars, and cannulae in a fitted case. Designed by Robert and Collin per Dieulafoy’s specifications.
1870 – Dieulafoy publishes De l’Aspiration pneumatique sous-cutanée, detailing methodology and outcomes. Fifty cases of hydarthrosis and several cases of pleurisy are cited as successfully managed with his technique.
1873 – The aspirator is showcased at the Universal Exposition in Vienna, establishing international recognition.
The Dieulafoy aspirator continued to be manufactured until 1940.
Dieulafoy’s Triad [DUAL USAGE]
Dieulafoy described two clinically significant triads: one in hysterical (functional) blindness and one in acute appendicitis. These diagnostic triads appear in his lectures and case reports from the Hôtel-Dieu hospital (1898-1904) and commonly cited in early 20th-century medical literature.
Dieulafoy’s Triad (Appendicitis) [Triade de Dieulafoy]
Triad of physical findings indicating acute appendicitis outlined by Dieulafoy to differentiate appendicitis from intestinal lithiasis and other causes of abdominal pain.
- Cutaneous hyperaesthesia (hyperesthésie cutanée)
- Involuntary muscular guarding (défense musculaire)
- Tenderness at McBurney’s point (douleur au point de Mac-Burney)
Original
English
Au cas d’appendicite, le territoire abdominal cutané, qui correspond à la zone douloureuse sous-jacente, est le siège d’une hyperesthésie caractéristique et le plan musculaire abdominal est tendu, douloureux, contracturé au point de Mac-Burney…c’est à cette région que se localisent l’hyperesthésie cutanée et la défense musculaire, qui sont des éléments précieux de diagnostic.- Dieulafoy 1898
In cases of appendicitis, the abdominal cutaneous area, which corresponds to the underlying painful area, is the site of characteristic hyperesthesia, and the abdominal muscles are tense, painful, and contracted at the MacBurney point.
…it is in this region that cutaneous hyperesthesia and muscular guarding are located, which are valuable diagnostic elements. – Dieulafoy 1898
Dieulafoy’s Triad (functional blindness) [triade symptomatique de la cécité hystérique]
Triad suggestive of functional/hysterical blindness described by Dieulafoy in his clinical lectures at Hôtel-Dieu de Paris.
- Sudden onset of blindness (cécité à début brusque)
- Preserved pupillary light reflexes (conservation des réflexes pupillaires)
- Normal fundoscopic exam (intégrité du fond de l’œil)
Original
English
Cécité complète à début brusque, conservation du réflexe pupillaire à la lumière et intégrité du fond de l’œil… ces constatations répondaient au syndrome que je désigne du nom de ‘triade symptomatique de la cécité hystérique.’ – Dieulafoy 1904
Complete blindness with sudden onset, preservation of the pupillary light reflex, and integrity of the fundus… these findings corresponded to the syndrome that I call the ‘symptomatic triad of hysterical blindness.’ – Dieulafoy 1904
Confirmed and cited by Crouzon (1915) in wartime neuropsychiatric observations of sudden blindness without organic findings. Multiple cases published e.g. cécité temporaire provoquée par l’éclatement d’obus à proximité
Major Publications
- Dieulafoy G. De La mort subite dans la fièvre typhoïde. Thèse de doctorat. Masson, Paris, 1869
- Dieulafoy G. De l’Aspiration pneumatique sous-cutanée, méthode de diagnostic et de traitement,. English translation: On sub-cutaneous pneumatic aspiration, as a method of diagnosis and of treatment. 1870 [Dieulafoy’s aspirator]
- Dieulafoy G. Traité de l’aspiration des liquides morbides. English translation: A treatise on the pneumatic aspiration of morbid fluids]. 1873
- Dieulafoy G. De la thoracentése, par aspiration dans la pleurésie aiguë. 1878
- Dieulafoy G. La tuberculose expérimentale chez le singe. 1883.
- Dieulafoy G. Manuel de pathologie interne. 1896
- Dieulafoy G. Exulceratio simplex. L’intervention chirurgicale dans les hématémèses foudroyantes consécutives à l’exulcération simple de l’estomac. Bulletin de l’Académie nationale de médecine 1898; 39: 49-84.
- Dieulafoy G. Clinique médicale de l’Hôtel-Dieu de Paris 1898-1909 (Vol II, III, IV, V, VI)
- Dieulafoy G. Lithiase intestinale et entéro-colite. Clinique médicale de l’Hôtel-Dieu de Paris, 1898: I: 296 [trois signes caractéristiques de l’appendicite]
- Dieulafoy G. Exulceratio simplex, hématémèses foudroyantes guéries par intervention chirurgicale. Clinique médicale de l’Hôtel-Dieu de Paris, 1898: II.
- Dieulafoy G. Deux case de cécité hystérique. Clinique Médicale de l’Hôtel-Dieu de Paris, 1904; V: 75 [triade symptomatique de la cécité hystérique]
References
Biography
- Peumery JJ. Georges Dieulafoy (1839-1911) et l’enseignement de la médecine à Paris à la charnière du Second Empire et de la IIIe République. Vesalius. 2004 Dec;10(2):74-7.
- de Parades V, Zeitoun JD, Fathallah N. et al. Georges-Paul Dieulafoy (1839-1911) de l’ulcération…Colon Rectum 2017; 11: 49–51
- Fresquet JL. Georges Paul Dieulafoy (1839-1911). Historia de la Medicina
- Georges Dieulafoy (1839-1911). BNF
- Peschanski N, Cadogan M. A vivid grouping (1903). LITFL
Eponymous terms
- Corput BE. Note sur un nouveau trocart aspirateur [trocart universal] destiné a pratiquer en même temps l’exploration, l’évacuation et injection. Bulletin de l’Académie royale de médecine de Belgique, 1856; 15: 537-542
- Gubler. M. Un aspirateur sous-cutané destiné au diagnostic et au traitement des collections liquides profondes, et construit par MM. Robert et Colin sur les indications de M. le docteur G. Dieulafoy. Gazette hebdomadaire de médecine et de chirurgie 1869; 45: 708
- Gallard T. Anéurismes miliaires de l’estomac, donnant lieu à une hématémèses mortelle. Bulletin et mémoires de la Société médicale des hôpitaux de Paris, 1884; 1: 84-91.
- Crouzon O. Cécité temporaire provoquée par l’éclatement d’obus à proximité. Bulletins et mémoires de la Société médicale des hôpitaux de Paris. 1915; 39: 57-59 [hysterical blindness]
- Crouzon O. Shell-shock ; burial ; blow on occiput : Blindness. Shell-Shock and Other Neuropsychiatric Problems. 1917: 373
- Lee YT, Walmsley RS, Leong RW, Sung JJ. Dieulafoy’s lesion. Gastrointest Endosc. 2003 Aug;58(2):236-43.
- Baxter M, Aly EH. Dieulafoy’s lesion: current trends in diagnosis and management. Ann R Coll Surg Engl. 2010 Oct;92(7):548-54.
- Karamanou M, Fiska A, Demetriou T, Androutsos G. Georges-Paul Dieulafoy (1839-1911) and the first description of “exulceratio simplex”. Ann Gastroenterol. 2011;24(3):188-191.
- Senger JL, Kanthan R. The Evolution of Dieulafoy’s Lesion Since 1897: Then and Now-A Journey through the Lens of a Pediatric Lesion with Literature Review. Gastroenterol Res Pract. 2012;2012:432517.
- Kolli S, Dang-Ho KP, Mori A, Gurram K. The Baader-Meinhof Phenomenon of Dieulafoy’s Lesion. Cureus. 2019 May 3;11(5):e4595.
- Talia FM, Fatima A. Dieulafoys Lesion Causing Gastrointestinal Bleeding. National Library of Medicine, StatPearls, 2023.
Eponym
the person behind the name

MBBS Newcastle University, UK. Currently working at Sir Charles Gairdner Hospital, Perth. Aspiring anaesthetist
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |