
![]()
Herbert M. Greene

Herbert Merton Greene (1878-1962) was an American physician
Greene was a University of Oregon Medical School graduate, and Army Medical Corps officer who served in the Mexican Expedition and as chief surgeon at Camp Lewis during World War I and the 1918 influenza pandemic.
Greene is remembered for his early work on dural trauma, CSF leakage, and prevention of post-lumbar puncture headache. He proposed that headache after lumbar puncture resulted from persistent CSF leakage through the dural puncture site, especially after using larger cutting needles.
His proposed solution was the Greene needle a small, smooth, round-pointed lumbar puncture needle designed to pass between longitudinal dural fibres rather than cut them. Greene’s microphotographs of experimental dural punctures showed smaller slit-like openings with round-pointed needles and larger flap-like defects with bevelled cutting needles.
Biographical Timeline
- Born on October 5, 1878 in Spruce Pine, Mitchell, North Carolina son of Jesse R. Greene and Helen A. Wiseman
- 1904 – Graduated MD, University of Oregon Medical School.
- 1900s–1910s – Practised medicine in the Pacific Northwest, associated with the Oregon medical community.
- 1916 – Served with the Army Medical Corps during the Mexican Expedition.
- 1917–1918 – Served during the First World War as chief surgeon at Camp Lewis, Washington during the influenza pandemic; rose to rank of Colonel.
- 1918 – Worked at Camp Lewis, Washington, during the influenza pandemic.
- 1923 – Published “A technic to reduce the incidence of headache following lumbar puncture in ambulatory patients with a plea for more frequent examination of cerebrospinal fluids”
- 1926 – Published “Lumbar puncture and the prevention of postpuncture headache” in JAMA.
- 1920s–1930s – Continued medical practice and publication in Oregon.
- 1956 – Awarded the University of Oregon Medical School Alumni Association Citation of Meritorious Achievement at the annual banquet in Portland, recognising “more than half a century of service and sacrifice to the alleviation of human suffering.”
- Died March 22, 1962 in Portland, Oregon, aged 83, from metastatic lung carcinoma
Medical Eponyms
Greene needle and prevention of post-puncture headache
Greene’s major contribution was the early recognition that post-lumbar puncture headache was related to dural trauma and leakage of cerebrospinal fluid. In 1923 he studied experimental punctures in spinal dura using needles of different sizes and tip shapes, then examined the resulting defects microscopically. He concluded that large cutting needles destroyed longitudinal dural fibres, produced larger openings, and allowed persistent CSF leakage.
Greene illustrated his argument with microphotographs of spinal dura punctured by different needles. The small round-pointed needle produced a narrow slit-like opening, while larger bevelled cutting needles produced broad flap-like defects, especially when the cutting edge crossed the longitudinal dural fibres. He concluded that larger dural wounds allowed more persistent CSF leakage.
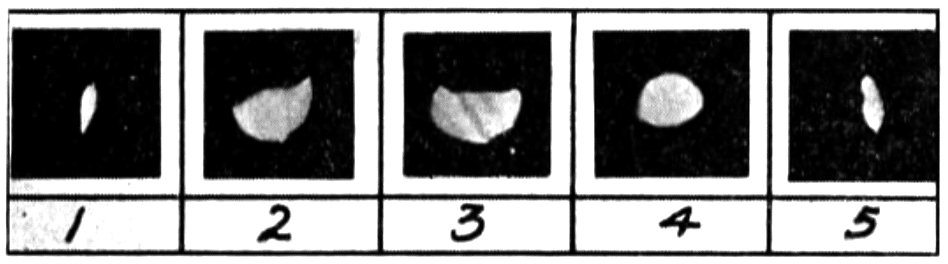
2. Gauge No. 18 needle with beveled cutting end. Cutting transverse to the dural fibres. Semicircular flap and destruction of dural fibres.
3. Gauge No. 18 needle with beveled cutting end. Cutting longitudinal with dural fibres. Semicircular flap with dural fibres severed in two places
4. Gauge No. 20 needle. Cutting transverse to dural fibres. Same flap as (2) but smaller
5. Gauge No. 20 needle with end sharpened to a round sharp point to remove all cutting edges. Cutting transverse to the fibres of the dura.
To reduce this trauma, Greene advocated a fine, round-pointed lumbar puncture needle. Rather than cutting the dura, the rounded point was intended to pass between dural fibres, which would then approximate after withdrawal of the needle. He recommended a No. 26 needle where possible, though he noted that a No. 23 needle was easier to manipulate in practice.
Greene needle
The Greene needle was a fine lumbar puncture needle with a rounded, tapering, non-cutting point. The needle was designed to separate longitudinal dural fibres rather than incise them. The needle preceded the pencil-point spinal needle design, without closed conical tip and lateral orifice of the Whitacre or Sprotte needles.

Controversies
Herbert Merton Greene described a small round-pointed lumbar puncture needle to reduce post-puncture headache in 1923 (Greene needle). This should be kept distinct from Barnett Alan Greene (1907–1999), who later described a 26G lumbar puncture needle passed through a 21G introducer for obstetric spinal analgesia in 1950.
Major Publications
- Greene HM. A technic to reduce the incidence of headache following lumbar puncture in ambulatory patients with a plea for more frequent examination of cerebrospinal fluids. Northwest Medicine 1923; 22(7): 240–5
- Greene HM. Lumbar puncture and the prevention of postpuncture headache. JAMA. 1926; 86(6): 391-392.
References
Biography
- Herbert M. Greene. Northwest Medicine 1962: 522
- Portrait: Herbert M. Greene, M.D. (1878-1962). OHSU digital collection
- Herbert M. Greene, M.D., (1878-1962) cataracts, attributed to radiation exposure. OHSU digital collection
Eponymous terms
- Harms R, Cadogan M. History of Spinal Needles. LITFL
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |