
![]()
Hypercyanotic Episodes in the Newborn
aka Pediatric Perplexity 003
A 26 day-old baby boy has been brought to the emergency department by ambulance. The past few days he has had poor feeding and recurrent episodes of respiratory distress associated with ‘turning blue’.
He was diagnosed with Tetralogy of Fallot antenatally and was born at term (a normal vaginal birth). An echocardiogram 2 days after he was born confirmed the diagnosis – it also showed that his ductus arteriosus had closed. He was discharged from hospital 4 days after he was born.
On presentation, the baby is agitated, tachycardic, tachypneic and profoundly cyanotic.
Q1. What is Tetralogy of Fallot?
Answer and Interpretation
Tetralogy of Fallot (TOF) is a constellation of four cardiac abnormalities that results from a single developmental defect, namely, failure of the subpulmonic conus to expand. TOF accounts for about 10% of congenital heart disease.
The four characteristic abnormalities of TOF are:
- right ventricular hypertrophy (RVH)
- right ventricular outflow tract obstruction (RVOTO)
- ventricular septal defect (VSD)
- the presence of an over-riding aorta (dextroposed aorta)

These defects result in decreased pulmonary flow and right-to-left shunt through the VSD. Age of presentation and severity of cyanosis is largely determined by the severity of RVOTO — cyanosis may not be present at birth. In a neonate with a patent ductus arteriosus (PDA) an infusion of prostaglandin E1 can be used to prevent closure of the ductus, thus maintaining pulmonary blood flow via a left-to-right shunt from the aorta.
Q2. What is the likely diagnosis?
Answer and Interpretation
A hypercyanotic episode, aka a ‘tet spell‘.
These are severe cyanotic spells that typically occur in children with TOF. They can also occur with other cyanotic cardiac lesions.
Q3. Describe the underlying pathophysiology?
Answer and Interpretation
Management of ‘tet spells’ makes sense if you understand the underlying pathophysiology.
‘Tet spells’ may be spontaneous or precipitated by events associated with decreased systemic vascular resistance, such as:
- tachycardia
- hypotension
- exertion during feeding
- defecation
- crying
This leads to a vicious cycle, that is usually self-limiting (often only 15 to 30 minutes long) but may ultimately result in seizures, stroke or even death.

Q4. What cardiac murmur would you expect to hear during this episode?
Answer and Interpretation
Children with TOF typically have a right ventricular outflow tract obstruction murmur. During a ‘tet spell’ this murmur may become inaudible as blood flows through the VSD rather than the right ventricular outflow tract. There is also a loud and single S2 in TOF.
Right ventricular outflow tract obstruction murmur:
- Harsh systolic crescendo decrescendo murmur usually heard along the left mid- to upper sternal border with posterior radiation
VSD murmur:
- Harsh pansystolic murmur maximal at, and almost confined to, the lower left sternal edge. It is louder on expiration and when the defect is small.
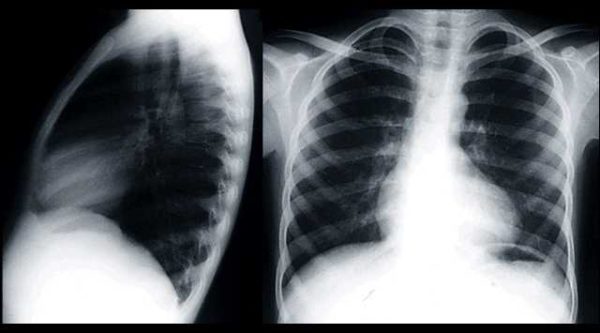
Q5. What are the classic chest x-ray findings in Tetralogy of Fallot?
Answer and Interpretation
The ‘boot-shaped’ heart.
Although heart size is usually normal it is classically ‘boot-shaped’ (coeur en sabot). There is a prominent right ventricle with decreased pulmonary vascularity.
Q6. Describe the initial management of this episode.
Answer and Interpretation
The main objectives are to increase systemic vascular resistance, correct hypoxia and correct acidemia.
To achieve this:
- Adminster high-flow oxygen via mask or head box – (decreases pulmonary vascular resistance)
- Avoid exacerbating distress, and remove identifiable precipitants (e.g. any cause of pain)
- Console the child by cradling in a knee–chest position. Squatting may be effective in older children. – (increases systemic vascular resistance)
- Adminster opioids in severe cases: eg. morphine 0.2 mg/kg IM. This relives distress and helps abolishes hyperpnea, but may worsen the loss of systemic vascular resistance.
- Other options include: midazolam, fentanyl, ketamine 1-2 mg/kg IV Initiate continuous ECG and oxygen saturation monitoring, frequent BP monitoring.
- Correct any underlying causes such as arrhythmia, hypothermia, hypoglycaemia.
Despite the initial measures describe in Q6, the baby remains distressed and profoundly cyanotic.
Q7. Describe the further management of a prolonged episode.
Answer and Interpretation
Therapeutic options for prolonged ‘tet spells’ include:
- IV fluids: 0.9% NaCl 10 mL/kg bolus followed by maintenance fluids. (increases venous return and may decrease heart rate)
- Correction of acidosis: sodium bicarbonate 1–2 mmol/kg IV (ensure adequate ventilation)
- Beta-blockers, (decreases heart rate and relieves infundibular spasm)
- IV esmolol: 0.5 mg/kg over 1 min, then 50–200 mcg/kg/min up to 48 h
- or propanolol: 0.01-0.2 mg/kg IV
- Vasopressors to increase systemic vascular resistance, promoting the redirection of blood flow through the pulmonary circulation:
- phenylephrine: 0.01-0.02 mg/kg IV
- or metaraminol 0.01 mg/kg stat, then 0.1-1 mcg/kg/min
- or noradrenaline 0.1-0.5 mcg/kg/min
- Manual compression of the aorta has also been described.
- Intubation and positive pressure ventilation may be required in extreme cases.
This case is continued in Cardiovascular Curveball 009…
References
- Costello JM, Almodovar MC. Emergency care for infants and children with acute cardiac disease. Clin Ped Emerg Med 8:145-155; doi:10.1016/j.cpem.2007.06.005
- Duncan A, Croston E. Guidelines for Intensive Care Management of Infants and Children after Congenital Heart Surgery. Pediatric Intensive Care Unit, Princess Margaret Hospital, 2008.
- Libby P, et al. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine (8th edition), Saunders Elsevier, 2008.
- Steinhorn RH. Evaluation and management of the cyanotic neonate. Clin Pediatr Emerg Med. 2008 Sep;9(3):169-175. PMID: 19727322; PMCID: 2598396
- van Roekens CN, Zuckerberg AL. Emergency management of hypercyanotic crises in tetralogy of Fallot. Ann Emerg Med. 1995 Feb;25(2):256-8. PMID: 7832359.

CLINICAL CASES
Paediatric Perplexity
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
