
![]()
Ivan Magill

Sir Ivan Whiteside Magill (1888 – 1986) was an Irish Anaesthetist.
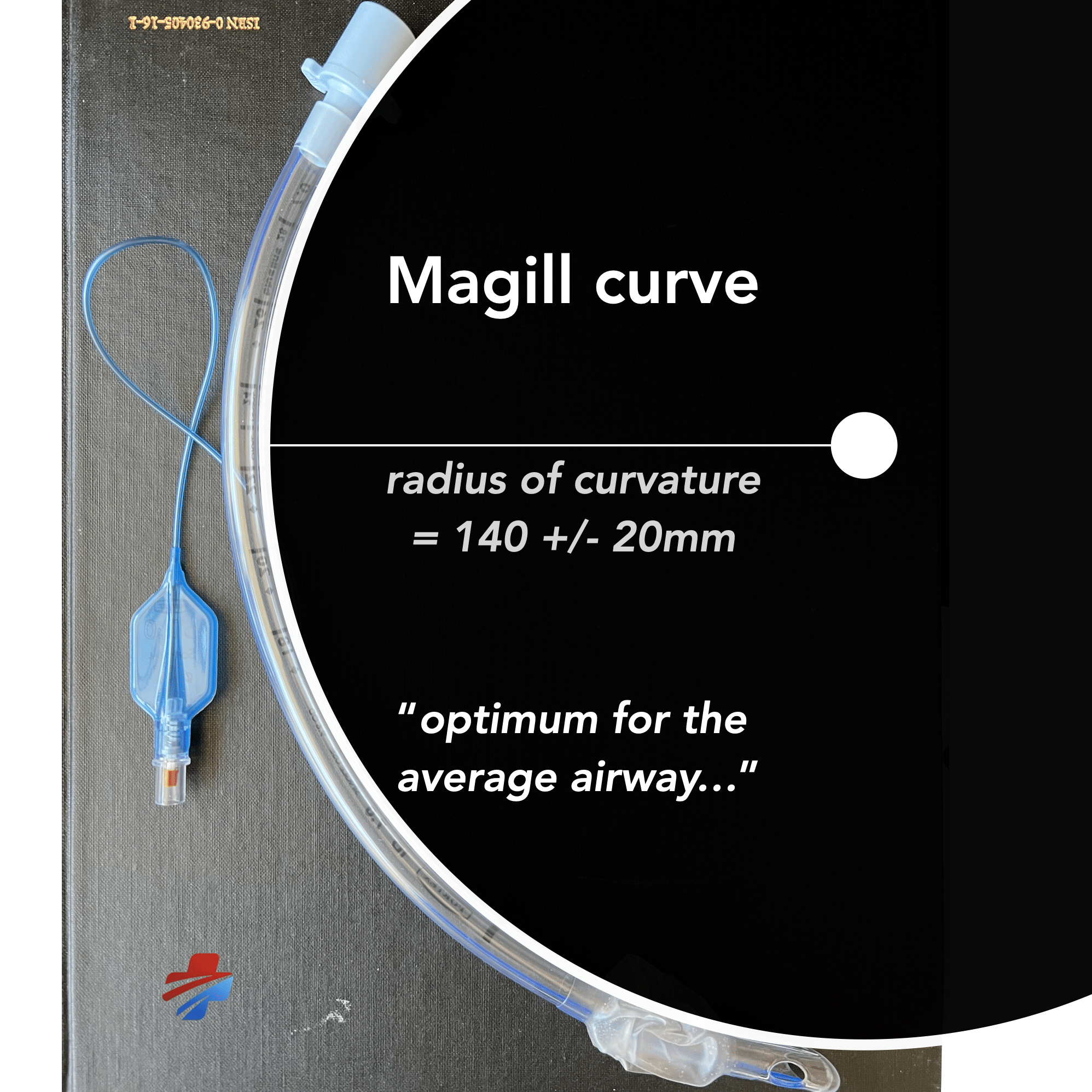
Magill was responsible for the modern endotracheal tube. Magill and his assistant cut the tubes used for research from a roll of rubber tubing. The tubing inherited the memory of the cylindrical roll and Magill relied on this natural curvature to avoid the use of metal stylet. This curvature of the endotracheal tube is still referred to as the “Magill Curve” [radius of curvature 140 ± 20mm]
Magill developed the technique of awake blind nasotracheal intubation and various anaesthetic devices including the Magill intubating forceps (1921); Magill laryngoscope blade (1926); apparatus for the administration of volatile anaesthetic agents (1927) and the Magill endotracheal tube (1920-1939).
Biography
- Born on July 23, 1888 in Larne, Ireland
- 1913 – MB BCh BAO, Queens University Belfast. Completed training in anaesthesia, which at the time was administration of an anaesthetic to a single patient. Magill commented that it was ‘inadequate training’.
- 1914-1918 Royal Army Medical Corps during World War I.
- 1919 – Anaesthetist at the Facial and Jaw Injury Hospital in Kent, where he developed the Magill forceps.
- 1920 – Queens University Belfast rejected Magill’s MD thesis on endotracheal anaesthesia, as it considered this unlikely to be of much value.
- 1935 – Instrumental in establishing the Diploma of Anaesthesia and was a founder member of Faculty of Anaesthesia of the Royal College.
- 1937 – Anaesthetist to Duchess of Gloucester during miscarriage.
- 1938 – Henry Hill Hickman Medal
- 1939-1945 Consultant to Amy, Navy and Emergency Medical Service.
- 1945 – Anaesthetist during Princess Margaret’s appendicectomy.
- 1946 – Commander of the Victorian Order (CVO)
- 1948 – FFARCS
- 1955 – Anaesthetist during Duke of Windsor’s detached retina surgery.
- 1966 – Knighted (KCVO)
- Died on November 25, 1986
Medical Eponyms
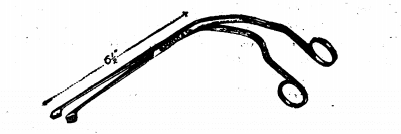
Magill forceps (1920)
Twin-bladed tong-like forceps. Rounded ends for grasping oblique angle between handles and blades to enable prevent obscuration of the view of the airway during use. Developed his forceps while working at the Queen’s Hospital for Facial and Jaw Injuries in Kent to aid in lifting and guiding the nasotracheal tube into the larynx. Magill published in 1921 BMJ:
Following on Dr. Rowbotham’s article in the Journal of October 16th on intratracheal anaesthesia by the nasal route, the accompanying illustration of a forceps, made for me by Messrs. Meyer and Phelps for a similar purpose, may be of interest. The forceps are constructed with a bend to clear the field of vision, as in Heath’s nasal forceps, the ends-which grasp the catheter representing a cylinder split longitudinally and serrated on the inner surface. Introduction of the catheter into the trachea is carried out with the aid of an electrically illuminated speculum, as in Dr. Rowbotham’s method, but I find in the forceps the following advantages over Dr. Rowbotham’s guiding rod:
- There is no injury to the end of the catheter, and therefore no liability of small pieces of the friable material being left in the trachea.
- The catheter is more easily picked up in the oral pharynx, and once grasped the hold is secure, without the necessity of holding the free end Which protrudes from the nose, as is the case with the guiding rod.
- The forceps can be used at the side of, as well as inside, the speculum.
- The field of vision is always clear.
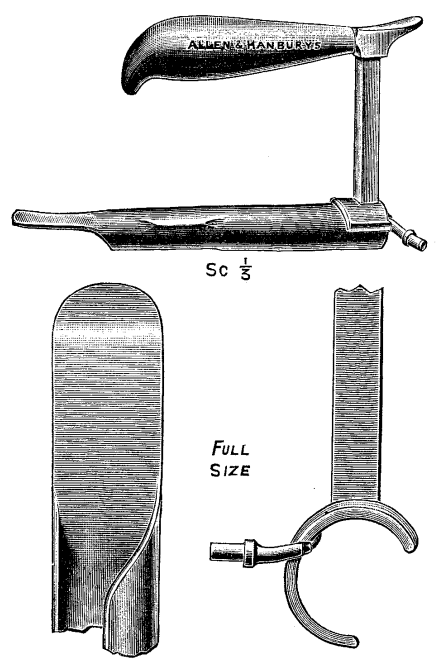
Magill laryngoscope (1926)
Magill laryngoscope blade pre-dates the 1941 Miller straight-blade. The Magill blade was a straight-blade, with a U-shaped step and flange concave to the right. The step and flange continued to within an inch of the end of the blade.
The laryngoscope here illustrated, although conforming in general outline to other similar patterns, embodies certain features which have proved useful in passing catheters and their accompanying expiratory tubes through the larynx. These are: (1) efficient illumination from a lens-fronted electric bulb of the size usual in sigmoidoscopes; (2) the distal end of the speculum is flat, wide, and tilted slightly upwards-an advantage in elevating and controlling the epiglottis; (3) the unusual width of the slot at the side facilitates the passing of catheters and tubes for expiration without obscuring the visual field; (4) the lug at the proximal end of the handle affords a purchase for the thumb, which is of value in manipulating the instrument into position. The handle is not detachable, and the barrel, which is polished within as well as without, is constructed of stainless steel.
Magill 1926
Magill anaesthetic apparatus (1927)
The illustration represents the fusion into one composite unit of an endotracheal ether insufflation apparatus and a nitrous-oxide and oxygen apparatus, both of which have been already described in the Lancet 1921 and Lancet 1923. The essential features of each have been retained with slight modifications as follows: (1) The unit is mounted upon a metal base, 9 inches by 6 inches, and can be carried in a bag without being dismantled. (2) The mechanical safety-valve and manometer are now fitted directly on the heating chamber. (3) The ether drop-feed has been altered to the shape of a dome which can be easily seen from any angle. (4) A water- sight-feed has been included for the administration of carbon dioxide.
Magill 1927

Magill curve (1928)
Magill and his assistant cut the tubes used for research from a roll of rubber tubing. The tubing inherited the memory of the cylindrical roll and Magill relied on this natural curvature to avoid the use of metal stylet. This curvature of the endotracheal tube is still referred to as the “Magill Curve” [radius of curvature 140 ± 20mm]
Research suggests the curve is ‘about optimum’ for the average airway.
Original description in 1928 pertains to ‘blind’ nasotracheal intubation – but the curve has been successfully applied to orotracheal tubes.
The ease with which “blind ” intubation can be carried out is purely a matter of anatomical consideration. In the normal subject, if the head be placed in the position which gives the freest nasal air-way–that is to say in a position of slight extension-the course of the air-way from the nostril to the glottis is a gentle curve, and a rubber tube with a similar curve, or a catheter mounted on a curved stilette, can naturally be made to follow that course and enter the glottis. In fact, with the head in the correct position in relation to the body, the tube will enter the glottis more readily than the oesophagus.
Magill 1928
Magill endotracheal tube (1920-1939)
Evolution of a series of endotracheal and endobronchial tubes with single and double lumens for various operative procedures. His 1939 ETT was stated to be so well made it may be passed through the nose, following the technique of Dr R. Tovell (Anesthesia and Analgesia (1937) 16, 105) and included is Dr Langton Hewer’s pilot balloon.
The Sir Ivan Magill Gold Medal (1988)
In 1988, to commemorate the centenary of his birth, the Association of Anaesthetists introduced the Sir Ivan Magill Gold Medal award for uniquely outstanding innovation in anaesthesia.
Winners of the award have shown extraordinary originality in developing the specialty of anaesthesia, through research, publications, technology, and more. Cast in gold, the medal includes a portrait of Sir Ivan, as well as the winner’s name and date of the award.
Major Publications
- Magill I. Forceps for intracheal anaesthesia. Br Med J 1920; 2: 670 [Magill forceps]
- Rowbotham ES, Magill I. Anaesthetics in the plastic surgery of the face and jaws. Proc R Soc Med 1921; 14:17-27
- Magill I. A Portable Apparatus for Tracheal Insufflation Anaesthesia. Lancet. 1921; 197(5096): 918
- Magill I. The provision for expiration in endotracheal insufflations anaesthesia. Lancet 1923; 202(5211): 68–9.
- Magill I. An apparatus for the administration of nitrous oxide, oxygen, and ether. Lancet.1923; 202(5214): 228.
- Magill I. An improved laryngoscope for anaesthetists. Lancet. 1926; 207(5349): 500 [Magill laryngoscope]
- Magill I. Improved anaesthetic apparatus. Lancet. 1927; 210(5425): 396
- Magill I. Endotracheal Anæsthesia. Proc R Soc Med. 1928; 22(2): 83–88.
- Magill I. Technique in endotracheal anaesthesia. BMJ. 1930; 2: 817–9.
- Langton Hewer C, Magill I. Discussion on anaesthesia in thoracic surgery. Proc R Soc Med 1930; 23: 643
- Magill I. Anaesthesia in thoracic surgery with special reference to lobectomy. Proc R Soc Med 1936; 29: 643
- Magill I. Endotracheal anaesthesia. Am J Surg. 1936; 34(3): 450-455.
- Magill I. Endotracheal tube with inflatable rubber cuff. Medical Annual. 1939; 57: 27 [Magill ETT]
- Magill I. An appraisal of progress in anaesthetics. Ann R Coll Surg Engl. 1966; 38: 154–65.
- Magill I. The heritages of the past are the privileges of the future. Anaesthesiology. 1967; 28(1): 202–8
- Magill I. Blind nasal intubation. In: Lest we forget. Anaesthesia. 1975; 30(4): 476–490
References
Biography
- Thomas KB. Sir Ivan Whiteside Magill, KCVO, DSc, MB, BCh, BAO, FRCS, FFARCS (Hon), FFARCSI (Hon), DA. Anaesthesia, 1978; 33(7): 628-634.
- Baskett P. The Resuscitation Greats. Sir Ivan Whiteside Magill KCVO DSc (Hon) Resuscitation. 2003 Nov;59(2):159-62.
- McLachlan G. Sir Ivan Magill KCVO, DSc, MB, BCh, BAO, FRCS, FFARCS (Hon), FFARCSI (Hon), DA, (1888-1986) Ulster medical journal, 2008 Sep; 77(3): 146-152
- Maltby R. Sir Ivan Whiteside Magill. In: Notable Names in Anaesthesia. The Choir Press; 2013: 123-125
- Bibliography. Magill, Ivan. WorldCat Identities
Eponymous terms
- White GMJ. Evolution of endotracheal and endobronchial intubation. Brit. J. Anaesth. 1960; 32: 235
- Chandler M. Tracheal intubation and sore throat: a mechanical explanation. Anaesthesia. 2002 Feb;57(2):155-61.
- Bateman BT, Alston TA. Commonly used eponyms in anesthesia. J Clin Anesth. 2009 Feb;21(1):67-71
- Yartsev A. The endotracheal tube in detail. Deranged physiology
- Sir Ivan Magill Gold Medal. Association of Anaesthetists
- Magill Laryngoscope. The Wood Library-Museum
- McKennedy C. Magill curve – Eponym A Day. Instagram
- Adami F. History of cardiopulmonary resuscitation LITFL
[cite]
British doctor working in Emergency Department and exploring Western Australia