
![]()
J. Leonard Corning
James Leonard Corning (1855-1923) was an American neurologist.
Corning laid the foundations of neuraxial anaesthesia. He received scientific training in chemistry, physiology, and pathology at Stuttgart, Heidelberg, and Würzburg, developing a strong experimental orientation.
His interests spanned neurology, psychiatry, pain, and neurophysiology, and he developed a reputation as an innovative thinker willing to test new physiological ideas experimentally. He explored vascular theories of epilepsy, designed mechanical neurotherapeutic devices, and experimented with music as a treatment for nervous disease.
In 1885, inspired by Carl Koller and his discovery of cocaine’s local anaesthetic properties, Corning conducted experiments injecting cocaine near the lumbar spine in animals and a human subject. Although he misinterpreted the anatomical mechanism and likely produced epidural rather than intrathecal blockade, his work represents the first published demonstration of neuraxial drug-induced neural conduction block.
Biography
- Born August 28, 1855 in Stamford, Connecticut
- 1861 – Family relocated to Stuttgart, Germany at the onset of the American Civil War.
- 1870–1872 – Educated at River View Military Academy, Poughkeepsie, New York.
- 1872–1875 – Studied chemistry at the Stuttgart Polytechnic Institute under Hermann von Fehling (1812–1885)
- 1875–1878 – Medical studies in Germany: Physiology at Heidelberg University under Wilhelm Kühne (1837–1900) and Pathology at University of Würzburg under Eduard Rindfleisch (1836–1908)
- 1878 – Awarded Doctor of Medicine, Surgery, and Obstetrics at Würzburg; dissertation based on original experimental pathology involving animal and microscopic work.
- 1879–1881 – Postgraduate clinical tours in Vienna, Paris, and London
- 1880s – Returned to the United States and established medical practice in New York City, specialising in neurology and neurotherapeutics. Appointed consultant to multiple New York institutions, including state hospitals for nervous and mental disease.
- 1885 – Conducted experiments injecting cocaine between lumbar spinous processes in dogs and a human subject. He published “Spinal anaesthesia and local medication of the cord”, the first recorded description of neuraxial blockade.
- 1886 – Featured in Virginia Medical Monthly for his work on local and spinal anaesthesia.
- 1890s – Developed mechanical devices for jugular compression and vagal stimulation in epilepsy, based on prevailing theories of cerebral hyperaemia.
- 1899 – Published experimental work on music therapy and emotional modulation during sleep, among the earliest systematic investigations of its kind.
- 1900–1915 – Continued prolific publication in neurology, psychiatry, pain, and neurovascular physiology; authored multiple books and over 40 papers.
- Died August 25, 1923 at his summer residence in Morristown, New Jersey, aged 67.
Next to averting death, the most royal prerogative of the modern physician is the annihilation of pain.
Corning 1886
Key Medical Contributions
Neuraxial blockade (1885)
In 1885, Corning conducted a series of experiments injecting hydrochlorate of cocaine between the lumbar spinous processes in dogs and later in a human subject. He observed segmental sensory changes and motor effects in the lower limbs, publishing his findings in Spinal anaesthesia and local medication of the cord. These experiments constitute the first published description of the principle of neuraxial blockade.
Corning was motivated by contemporary anatomical knowledge of the interspinous venous plexus and deliberately targeted the interspinous space:
I decided to inject the anaesthetic between the spinous processes of the lower dorsal vertebras… numerous small veins (venae spinosæ) run down between the spinous processes of the vertebræ, and, entering the spinal canal, join the more considerable vessels of the plexus spinalis interna.
His aim was explicit and experimental rather than surgical:
I was bent upon abolishing reflex action and annulling sensory conduction in the cord.
In his first experiment, Corning injected 1.5 mL of 2% cocaine between the inferior dorsal spinous processes of a dog. Within five minutes he observed incoordination followed by weakness and anaesthesia of the hindquarters and the effects resolved completely within four hours. In a subsequent human experiment, Corning injected 2 mL of 3% cocaine at the T11–12 interspinous space, repeating the dose after an initial lack of effect. Ten minutes later, the subject reported that his legs felt “sleepy”, and Corning noted that painful electrical stimuli which provoked brisk reflexes in the upper limbs were “disregarded and barely perceived in the lower limbs”. No motor weakness or gait disturbance was observed.
Corning believed that the anaesthetic effect resulted from vascular absorption of cocaine into the spinal cord rather than direct neural exposure. However, modern reinterpretation of his technique strongly suggests that he produced an epidural (extradural) block, not an intentional intrathecal spinal anaesthetic. In particular the high dose, delayed onset, limited dermatomal spread, and absence of cerebrospinal fluid flow. Notably, Corning recorded that the human subject experienced headache and vertigo the following day, raising the possibility of inadvertent dural puncture and early post–dural puncture headache, though he reported no lasting adverse effects.
Corning himself remained cautious about the clinical implications of his observations:
Whether the method will ever find an application as a substitute for etherization… further experience alone can show. Be the destiny of the observation what it may, it has seemed to me, on the whole, worth recording
Although his anatomical interpretation was incorrect, Corning’s early experiments established the concept that drugs introduced near the spinal canal could selectively interrupt neural conduction.
Regional anaesthesia (1885)
Corning developed an early method of prolonged regional anaesthesia based on “incarceration” of local anaesthetic within a limb. By combining subcutaneous cocaine injection with proximal exsanguination and mechanical tourniquets of his own design (the Corning tourniquet and Corning clamp), he aimed to prevent systemic absorption and prolong neural exposure.
On September 19, 1885 Corning published On the prolongation of the anaesthetic effects of the hydrochlorate of cocaine when subcutaneously injected
When we shut off the blood from a portion of the body previously injected with a comparatively weak solution of the hydrochlorate of cocaine…we incarcerate the solution in the field of operation, and are consequently enabled to perpetuate those chemical changes in the sensory filaments which are necessary to a suspension of conduction – to the maintenance of a prolonged condition of anaesthesia.
Corning regional anaesthesia procedure for upper and lower limb blocks.
- Exsanguination: Esmarch elastic bandage (a) is wrapped around the limb from distal to proximal, with the limb elevated and the bandage held in continuous stretch (b)
- Application of anaesthetic: Multiple subcutaneous injections of 0.5-1.0% cocaine hydrochlorate injected with syringe (e)
- Incarceration of anaesthetic in the field of operation: Corning originally used the tourniquet of Esmarch, but converted to a tourniquet of his own design – the Corning tourniquet (c) and Corning clamp (d):
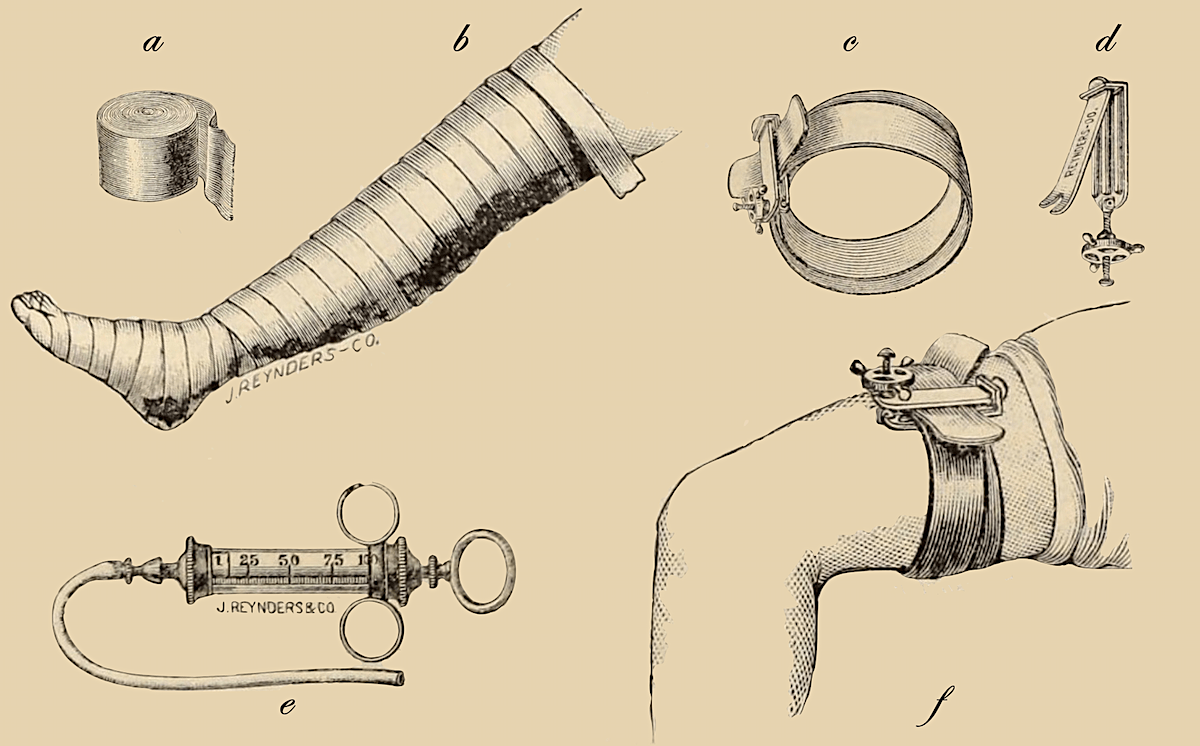
…an India-rubber band two inches broad and three feet long, the edges of which are nicely rounded. The tourniquet is applied around the limb above the anaesthetic zone in two or more folds, and secured in place by means of a powerful clamp of my own designing – It consists, in the first place, of two wings or blades, provided with round, ridge-like elevations on their inner surfaces. The two wings are joined at one end by means of a stout hinge, and at the other there is a powerful screw, which, being actuated by a milled wheel grasped by the hand of the operator, causes the jaws of the blades to close upon the folds of the India-rubber strap and hold the tourniquet securely in place (f)
Corning predicted the future of regional anaesthesia thus:
I feel certain that, we shall never be scientifically justified in dispensing with the precaution of incarceration by suspending the local circulation. My reason for this conviction is based upon the probability, almost amounting to a certainty, that any substance which possesses strong chemical affinity for the nerves must have like attraction for the complicated organic bodies which compose the central nervous system.
Corning 1885
Other Medical Contributions
Epilepsy devices and neurotherapeutics
Corning proposed a vascular theory of epilepsy, attributing seizures to cerebral hyperaemia. He designed mechanical devices for jugular compression and vagal stimulation to reduce cerebral blood flow and suppress seizures. Though these approaches were ultimately abandoned but demonstrated early experimentation with neuromodulation and non-pharmacological interventions for neurological disease.
Corning and Early Music Therapy
Corning was among the first to recommend music as a treatment for nervous disorders, particularly neurasthenia. He believed certain musical compositions could modulate cerebral activity, either exciting or soothing the mind.
Controversies
Priority: Corning vs Bier
A long-standing controversy concerns whether Corning or August Bier performed the first spinal anaesthetic. While Corning’s experiments clearly predate Bier’s 1898 intrathecal spinal anaesthesia, most modern historians agree that Corning did not intentionally or reliably enter the subarachnoid space. Bier therefore retains priority for the first confirmed intrathecal spinal anaesthetic used for surgery, whereas Corning is credited with establishing the experimental foundations of neuraxial blockade.
Misinterpretation of anatomy and mechanism
Corning misunderstood the mechanism of action of neuraxial cocaine, proposing that it reached the spinal cord via venous absorption rather than direct neural exposure. He also did not describe cerebrospinal fluid flow, which further supports an epidural rather than intrathecal injection. These errors limited immediate clinical adoption of his technique and contributed to later skepticism about his claims.
Major Publications
- Corning JL. Carotid compression and brain rest. 1882
- Corning JL. Brain-rest. 1883
- Corning JL. Brain exhaustion, with some preliminary considerations on cerebral dynamics. 1884
- Corning JL. Electrization of the sympathetic and pneumogastric nerves, with simultaneous bilateral compression of the carotids. New York Medical Journal 1884
- Corning JL. Spinal anaesthesia and local medication of the cord. New York Medical Journal 1885; 42: 483-485
- Corning JL. On the prolongation of the anaesthetic effects of the hydrochlorate of cocaine when subcutaneously injected. New York Medical Journal 1885; 42: 317-319
- Corning JL. Prolonged local anaesthetization by incarceration of the anaesthetic fluid in the field of operation. New York Medical Journal 1886; 43: 12-16. [Bier block]
- Corning JL. Local anæsthesia in general medicine and surgery, being the practical application of the author’s recent discoveries. 1886
- Corning JL. A further contribution on local medication of the spinal cord, with cases. Medical Record. 1888; 33: 291–3.
- Corning JL. A treatise on hysteria and epilepsy. 1888
- Corning JL. A treatise on headache and neuralgia. 1890
- Corning JL. Pain in its neuro-pathological, diagnostic, medico-legal, and neuro-therapeutic relations. 1894
- Corning JL. Experimental researches regarding the state of the mind in vertigo. New York Medical Journal 1895
- Corning JL. The Use of Musical Vibrations Before and During Sleep – Supplementary Employment of Chromatoscopic Figures – A Contribution to the Therapeutics of the Emotions. The Medical Record: A Weekly Journal of Medicine and Surgery, Medical Record. 1899(55): 79–86.
- Corning JL. The importance, both medico-legal and clinical, of the early recognition of certain organic affections of the nervous system, including paresis. 1900
- Corning JL. The Princess Ahmedée; a romance of Heidelberg. 1900 [Written under pseudonym: Roland Champion]
- Corning JL. The Musical Memory and Its Derangement (Amusia). Medical Record. 1912(81): 51–62.
References
Biography
- Biographical sketch of Doctor James Leonard Corning of New York City, and his recent remarkable discovery of local anaesthesia. Virginia Medical Monthly 1886; 12: 713–719.
- Gorelick PB, Zych D. James Leonard Corning and the early history of spinal puncture. Neurology. 1987 Apr;37(4):672-4.
- Bibliography. Corning, J. Leonard (James Leonard) 1855-1923. WorldCat Identities
Eponymous terms
- Marx GF. The first spinal anesthesia. Who deserves the laurels? Reg Anesth. 1994; 19(6): 429-30.
- Lanska DJ. J.L. Corning and vagal nerve stimulation for seizures in the 1880s. Neurology. 2002;58(3):452-9.
- van Zundert A, Helmstädter A, Goerig M, Mortier E. Centennial of intravenous regional anesthesia. Bier’s Block (1908-2008). Reg Anesth Pain Med. 2008; 33(5): 483-489.
- Davis WB. The first systematic experimentation in music therapy: the genius of James Leonard Corning. J Music Ther. 2012 Spring;49(1):102-17.
- Löser B, Petzoldt M, Löser A, Bacon DR, Goerig M. Intravenous Regional Anesthesia: A Historical Overview and Clinical Review. J Anesth Hist. 2019; 5(3): 99-108.
Eponym
the person behind the name

Doctor currently working in South Wales, training in anaesthetics. Graduated Leeds University with MB ChB with BSc in microbiology in relation to medicine. Special interests in emergency medicine, critical care and anaesthetics
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |