
![]()
James Paget
Sir James Paget (1814-1899) was an English surgeon
Paget was a surgeon, pathologist, medical educator and one of the leading figures of Victorian medicine. Based at St Bartholomew’s Hospital, London, he built his reputation through clinical observation and pathological correlation. He is most famous for his descriptions of Paget’s disease of the nipple, Paget’s bone disease and Paget-Schroetter Syndrome.
His wider work ranged across surgical pathology, tumour classification, bone disease, venous thrombosis, residual abscesses and recurrent fibroid tumours. As a medical student, he recognised the parasite later named Trichinella spiralis. His work contributed to descriptions of multiple diseases including neurofibromatosis, carpal tunnel syndrome, hereditary multiple exostosis, Osgood-Schlatter disease, and viruses in relation to cancers.
Biography
- Born on January 11, 1814, Great Yarmouth, Norfolk, England; eighth of seventeen children of Samuel and Sarah Elizabeth Paget
- 1830 – Apprenticed to Charles Costerton, surgeon, in Great Yarmouth. Practical exposure to surgery, dispensing, bleeding, record-keeping and local medical practice.
- 1834-1836 – Medical school at St Bartholomew’s Hospital, London. Observed the parasite later named Trichina spiralis (1835)
- 1836 – Qualified MRCS, Royal College of Surgeons of England.
- 1837-1842 – Sub-editor and contributor to the London Medical Gazette
- 1837 – Appointed curator of the museum at St Bartholomew’s Hospital.
- 1839 – Appointed Demonstrator in Morbid Anatomy at St Bartholomew’s.
- 1843 – Elected Fellow of the Royal College of Surgeons (FRCS). Lecturer in General Anatomy and Physiology and Warden of the newly created St Bartholomew’s Hospital Medical College.
- 1846-1849 – Prepared descriptive catalogues of the Anatomical Museum at St Bartholomew’s and the Pathological Museum at the Royal College of Surgeons
- 1847 – Appointed Assistant Surgeon at St Bartholomew’s. Arris and Gale Professor of Anatomy and Surgery at the Royal College of Surgeons
- 1851 – Elected Fellow of the Royal Society (FRS)
- 1853 – Published Lectures on Surgical Pathology
- 1858 – Appointed Surgeon Extraordinary to Queen Victoria; also published on upper-limb venous enlargement after exertion, later linked to Paget-Schroetter syndrome
- 1861 – Became full Surgeon at St Bartholomew’s Hospital.
- 1863 – Appointed Surgeon-in-Ordinary to the Prince of Wales.
- 1867 – Serjeant-Surgeon Extraordinary to Queen Victoria.
- 1871 – Awarded a Baronet by Queen Victoria, pronouncing him Sir James Paget. Consulting Surgeon at St Bartholomew’s
- 1874 – Published on disease of the mammary areola preceding cancer of the mammary gland, later known as Paget’s disease of the nipple
- 1875 – President of the Royal College of Surgeons.
- 1877 – Published on osteitis deformans, now Paget’s disease of bone; delivered the Hunterian Oration; became Serjeant-Surgeon to Queen Victoria.
- 1881 – President of the 7th International Medical Congress in London.
- 1883-1895 – Vice-Chancellor, University of London
- 1887 – First Morton Lecturer on cancer and cancerous diseases; President of the Pathological Society of London.
- Died on December 30, 1899, London, aged 85. Funeral held at Westminster Abbey on January 4, 1900.
Medical Eponyms
Paget-Schroetter syndrome [Paget 1858; 1875 and Schrötter 1884]
Paget-Schroetter syndrome (or effort thrombosis), is an axillo-subclavian vein thrombosis usually associated with repetitive activity of the upper limbs. In effect the thrombotic form of venous thoracic outlet syndrome.
1858 – Paget described “some affections of voluntary muscles as a consequence of excessive exercise.” Among his cases were examples of upper-limb enlargement associated with fullness of the superficial veins, suggesting obstruction of the axillary vein.
In another case, in a soldier 27 years old, there was great enlargement of all the muscles of the right arm and shoulder, and such fulness of all its subcutaneous veins, and such a feeling of weight and tightness when it hung down, that I supposed the axillary vein must be obstructed. However, with rest in the Hospital, and the occasional application of leeches, the muscles gradually diminished, and the veins be came less filled; and finally, during an attack of scarlatina, they returned to nearly their natural state.
Paget, Medical Times and Gazette. March 1858
1875 – Paget described in greater detail two of these cases in the chapter “gouty phlebitis” in his collection of Clinical lectures and essays. This account is often cited as his classic description of effort thrombosis, despite a clear reference to the original publication of the cases from March 1858.
In strong contrast with cases of widely diffused phlebitis, are those in which a single small portion of a great vein becomes obstructed…
A man about 50 years old, thin, and moderately muscular, and usually healthy, observed, during a September, that his right arm was growing larger, and, as he thought, stronger, and fitter for work…I found the upper arm two inches more in circumference than the left, and the whole limb enlarged in the same proportion.
With the help of the hot douche, warmth, and friction, the swelling of the arm very gradually subsided; and, as it did so, the cord-like feeling of the obliterated axillary vein became more distinct. A year elapsed before the vein regained its completely natural condition.
Paget, ‘Gouty Phlebitis’ 1875
1884 – Leopold von Schrötter (1837-1908) proposed the mechanism that thrombosis in a previously healthy vein caused by mechanical stress, especially unusual movement, pressure, or muscular strain.
1948 – Australian surgeon, Sir Edward Stuart Reginald Hughes termed the condition
The association of acute venous stasis and a healthy person constitutes a syndrome which, in the absence of unanimity of opinion as regards the aetiology or pathology, might well be called the ‘Paget-Schrotter syndrome’.
Hughes ESR, 1948
The term persists as Paget-Schroetter syndrome, Paget-Schrötter syndrome, or Paget-von Schrötter syndrome, alongside the descriptive term effort thrombosis.
Paget’s disease of the nipple (1874)
Paget’s disease of the nipple is an uncommon manifestation of breast malignancy presenting as an eczematous, erythematous, crusted, scaly, ulcerated or exudative lesion of the nipple–areola complex. It is usually associated with underlying ductal carcinoma in situ or invasive ductal carcinoma, although the visible lesion may be mistaken for benign eczema, dermatitis or psoriasis.
1840 – Originally described by Velpeau, the French surgeon failed to link physical manifestation to underlying breast cancer. Paget described the skin changes, and its underlying implications in cancer diagnosis.
1874 – Paget published On diseases of the mammary areola preceding cancer of the mammary gland in the St Bartholomew’s Hospital Reports. He reported about fifteen women, aged forty to sixty or older, in whom a chronic eruption of the nipple and areola preceded the development of scirrhous carcinoma of the breast.
Paget provided the clinical description:
The patients were all women, various in age from 40 to 60 or more years, having in common nothing remarkable but their disease. In all of them the disease begins as an eruption of the nipple and areola. In the majority it had the appearance of a florid, intensely red, raw surface, very fine and granular, as if nearly the whole thickness of the epidermis were removed; like the surface of very acute diffuse eczema, or like that of an acute balanitis. From such a surface, on the whole or greater part of the nipple and areola, there was always copious, clear, yellowish, viscid exudation. The sensations were commonly tingling, itching, and burning, but the malady was never attended by disturbance of the general health.
Paget recognised the temporal association with breast cancer:
But it has happened in every case which I have been able to watch, cancer of the mammary gland has followed within at the most two years, and usually within one year… The formation of cancer has not in any case taken place first in the diseased part of the skin. It has always been in the substance of the mammary gland, beneath or not far from the diseased skin, and always of a clear interval of apparently healthy tissue
Paget’s disease of bone (1877) [aka Paget disease; osteitis deformans]
Paget disease of bone (osteitis deformans) is a metabolic disorder of the bone, resulting in deformation and pain. It most commonly affects the axial skeleton with pelvis, lumbo-sacral spine, skull, femur and tibia.
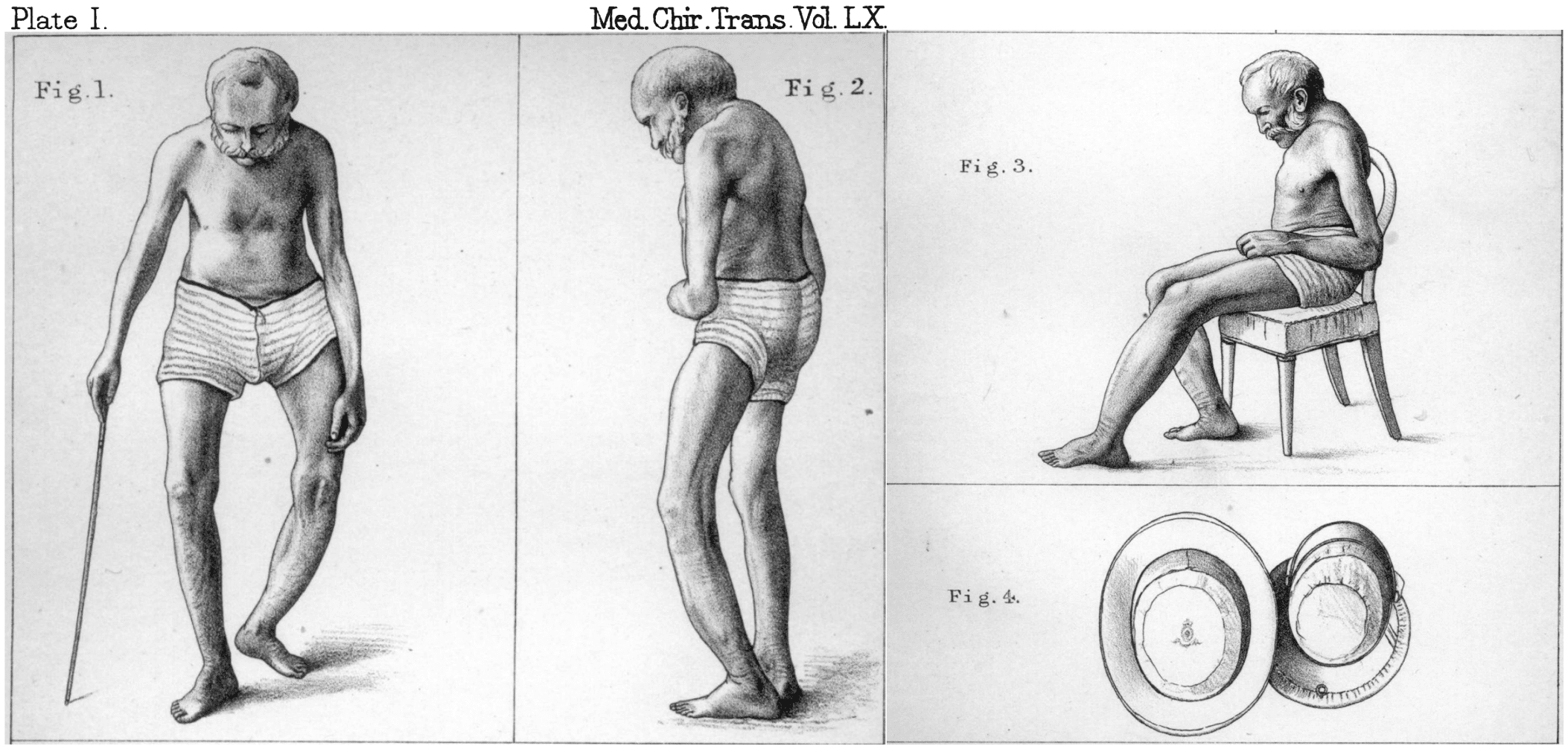
1876 – Paget first presented the condition to the Royal Medico-Chirurgical Society on November 14, 1876 (published in 1877) as On a Form of Chronic Inflammation of Bones (Osteitis Deformans). Paget described five patients, beginning with a man he had first seen in 1856, who developed slowly progressive enlargement and deformity of the skeleton. The most striking features were bowing of the long bones, enlargement of the skull, curvature and shortening of the spine, deafness, visual complications and, in some cases, later malignant disease of bone.
Paget provided the classic description of progressive bone enlargement and deformity:
The left femur and tibia became larger, heavier, and somewhat more curved. Very slowly those of the right limb followed the same course…
The skull became gradually larger, so that nearly every year, for many years, his hat, and the helmet that he wore as a member of a Yeomanry Corps needed to be enlarged.
The spine very slowly became curved and almost rigid. The whole of the cervical vertebrae and the upper dorsal formed a strong posterior, not angular, curve; and an anterior curve, of similar shape, was formed by the lower dorsal and lumbar vertebrae. The length of the spine thus seemed lessened, and from a height of six feet one inch he sank to about five feet nine inches.
Paget’s Recurrent Fibroid tumour (1853)
A fibroid-like soft tissue tumour that recurs locally after apparent complete excision. Paget used the term for tumours that resembled ordinary fibrous tumours grossly and microscopically, but behaved differently. These tumours returned repeatedly at or near the operative site, while lacking the usual features of cancer such as lymphatic spread, visceral deposits or cachexia.
In his Lectures on Surgical Pathology, Paget grouped these lesions between innocent and malignant tumours. He proposed the name “Recurrent fibroid tumours” for the form in which recurrence was most strongly shown.
We have in these recurrent tumours characters which connect them on the one hand with the innocent, and on the other with the malignant tumours, so that the plan I have adopted of placing them in a group intermediate between those two great divisions seems not inexpedient…the tumours which I have termed Recurrent Fibroid
The recurrence of these tumours takes place, not merely in the same organ or tissue, but in loco — in the place in which they originally occurred — in the cicatrix, or closely adjacent to the scar of the first operation wound. And here, again, do they possess a character by which they are distinguished from the malignant tumours, which in their recurrence may multiply not only in the same part but in distant organs.
Paget 1853
The term is historical, but the closest modern counterpart is desmoid-type fibromatosis, also known as aggressive fibromatosis.
Paget’s residual abscess (1869)
Paget’s residual abscess refers to delayed suppuration arising in or near the residue of a previous inflammatory process.
All abscesses formed in or about the residues of former inflammations
1869 – Paget published On Residual Abscesses in St Bartholomew’s Hospital Reports. He used the term for abscesses forming in old sites of disease, especially after spinal and disease, necrosis, scrofulous lymphadenitis or previous abscess. The swelling could appear years after apparent recovery, often with little pain, fever or constitutional disturbance, and could mimic a bursa or soft-tissue tumour.
Paget’s Test
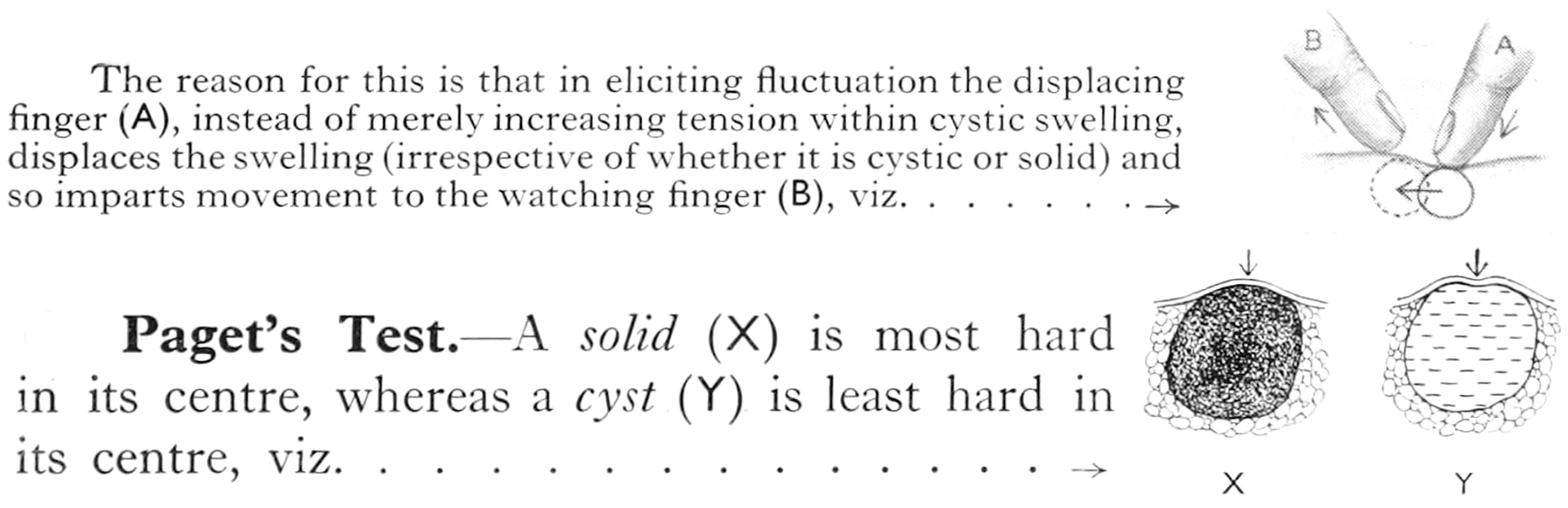
Paget’s test is a historical surgical examination test used to distinguish a small cystic swelling from a solid tumour. It is applied when ordinary fluctuation is difficult to elicit. A solid swelling is usually firmest at its centre, whereas a cystic swelling is least firm centrally because pressure displaces its fluid contents.
No original publication by Paget has yet been identified for this test. The eponymous term appears in later surgical teaching, particularly in relation to the examination of small superficial lumps. According to Hamilton Bailey, in swellings of less than ¾ in. (18 mm.) the sign of fluctuation is unreliable and Paget’s test should be applied.
Key Medical Contributions
Trichinella spiralis
As a first-year medical student at St Bartholomew’s Hospital, Paget observed small white specks in the muscles of a cadaver during dissection. Rather than dismissing them as incidental deposits, he examined them microscopically and recognised a minute coiled parasite. Richard Owen subsequently described and named the organism Trichina spiralis in 1835.
Another event, in this first year’s study, which had some influence on my later Hfe, was the discovery of the Trichina spiralis. Dr. Cobbold has told the story of the several steps leading to the discovery and following it, in his latest work on the Entozoa. My share was the detection of the ‘worm’ in its capsule; and I may justly ascribe it to the habit of looking-out, and observing, and wishing to find new things, which I had acquired in my previous studies of botany. All the men in the dissecting-rooms, teachers included, ‘saw’ the little specks in the muscles: but I beheve that I alone ‘looked-at’ them and ‘observed’ them: no one trained in natural history could have failed to do so.
Paget 1901
Paget made the original observation and prepared the material, but Owen supplied the formal zoological description and name. The organism was later renamed Trichinella spiralis by Alcide Railliet in 1895 because Trichina had already been assigned to an insect in 1830.
Osgood-Schlatter disease (1891)
Paget contributed to the history of Osgood-Schlatter disease with his description of painful tibial tubercle enlargement in athletic young people. His described the clinical pattern later associated with traction apophysitis of the tibial tubercle. Paget published periostitis following strains and described tibial tubercle enlargement in young athletes:
Much more common are the enlargements of the tubercle of the tibia which are often seen in young people much given to athletic games. They complain of aching pain at and about the part, especially during and after active exercise, and the tubercle may be felt enlarged and is often too warm. The pain often continues, more or less, for many months, and there may be enlargement of the bursa under the ligamentum patellae, and the tubercle may remain too prominent; but common as are these cases, especially in our public schools, I have never known grave mischief ensue in any of them, and they get well of themselves. They may represent one of the least degrees of periostitis due to strain; the increase of the prominence of the bone is only just beyond that which may be deemed the normal limit for the attachment of vigorous muscles.
Paget 1891
Carpal Tunnel syndrome
Paget provided an early description of median nerve compression at the wrist in his Lectures on Surgical Pathology (1853). He described two cases of median nerve injury. The first followed constriction at the wrist by a tight cord and the second followed fracture of the distal radius with excessive new bone formation and compression of the median nerve.
Paget did not define carpal tunnel syndrome but recognised the pathological effect of pressure on the median nerve at the wrist, and the clinical improvement when that pressure was relieved.
Major Publications
- Paget CJ, Paget J. Sketch of the natural history of Yarmouth and its neighbourhood. 1834
- Paget J. The motives to industry in the study of medicine. Delivered at Saint Bartholomew’s Hospital, on Thursday, October 1, 1846
- Paget J. Account of a dislocation, in consequence of disease of the first and second cervical vertebrae. Medico-Chirurgical Transactions 1848; 31: 285-95.
- Paget J. Lectures on tumours. Delivered in the Theatre of the Royal College of Surgeons of England. 1851
- Paget J. Lectures on surgical pathology: Delivered at the Royal College of Surgeons of England. 1853 [2e 1876]
- Paget J. On some affections of voluntary muscles III. Medical Times and Gazette. 1858; 260-261 [Paget-Schroetter syndrome]
- Paget J. On residual abscesses. St Bartholomew’s Hospital Reports. 1869; 5: 73–79.
- Paget J. What becomes of medical students. St Bartholomew’s Hospital Reports 1869; 5: 238–242.
- Paget J. On diseases of the mammary areola preceding cancer of the mammary gland. St. Bartholomew Hospital Reports, London, 1874, 10: 87-89. [Paget’s disease of the nipple]
- Paget J. Gouty Phlebitis. In: Clinical lectures and essays. 1875 [Paget-Schroetter syndrome p305-308]
- Paget J. On a Form of Chronic Inflammation of Bones (Osteitis Deformans). Medico-Chirurgical Transactions 1877;60:37-64 [Paget’s disease of bone]
- Paget J. The Hunterian oration. 1877
- Paget J. Additional cases of osteitis deformans, notes on seven cases. Medico-Chirurgical Transactions 1882; 65: 225-36 [Paget’s disease of bone]
- Paget J. The Hunterian oration. 1877
- Paget J. The Morton Lecture on cancer and cancerous diseases. Delivered at the Royal College of Surgeons of England on Friday, Nov. 11, 1887
- Paget J. An address on the utility of scientific work in practice. Br Med J 1887;2: 811-814
- Paget J. Studies of old case-books. 1891
References
Biography
- Paget S. Memoirs and letters of Sir James Paget. 1901
- Buchanan WW. Sir James Paget (1814-99): surgical Osler? Proc R Coll Physicians Edinb. 1996 Jan;26(1):91-114.
Eponyms
- Owen R. Description of a Microscopic Entozoon infesting the Muscles of the Human Body (Trichina spiralis). Proceedings of the Zoological Society of London. 1835; 3: 23–27.
- Turner G. The Paget tradition. New England Journal of Medicine, 1931;205: 622-629
- Campbell WC. History of trichinosis: Paget, Owen and the discovery of “Trichinella spiralis”. Bulletin of the History of Medicine. 1979; 53: 520–552.
- Buchanan W. The contribution of Sir James Paget (1814-1894) to the study of rheumatic disease. Clin Rheumatol. 1996 Sep;15(5):461-72.
- Colman E. Sir James Paget: the man and the eponym. Calcif Tissue Int. 2002 May;70(5):430-1.
- McManus IC. Sir James Paget’s research into medical education. Lancet. 2005 Aug 6-12;366(9484):506-13.
- Paget J. The first description of carpal tunnel syndrome. J Hand Surg Eur Vol. 2007 Apr;32(2):195-7.
- Tjalma WA, Bosteels J, Thiessen F, Smets K. Rewriting the history of Paget’s disease: From Arderne’s medieval case to Crocker’s first extramammary description (1370-1889). Eur J Obstet Gynecol Reprod Biol. 2026 Jun;322:115082.
- Rippey J. Ultrasound Case 085. LITFL
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |