
![]()
Ultrasound Case 085
Presentation
A 35 year old man presents with a swollen and uncomfortable right arm.


View 3: Axillary vein transverse
View 4: Longitudinal view axillary vein
View 5: Longitudinal view axillary and subclavian veins
View 6: Longitudinal view of subclavian vein

Describe and interpret these scans
IMAGE INTERPRETATION
Images 1 & 2: Clinical photo of upper limbs.
The patient is muscular. His right upper limb is plethoric and swollen. The superficial collateral veins over his upper arm and chest are prominent (Urschel’s sign). This is clinically almost certainly an upper limb deep venous thrombosis.
Image 3: Transverse image right axillary vein, moving medially toward the subclavian vein.
Partially occlusive thrombus is seen in the axillary vein. The axillary vein becomes the subclavian vein at the lateral margin of the first rib but disappears deep to the clavicle, the subclavian can then be interrogated from the supraclavicular approach to the junction with the internal jugular vein.
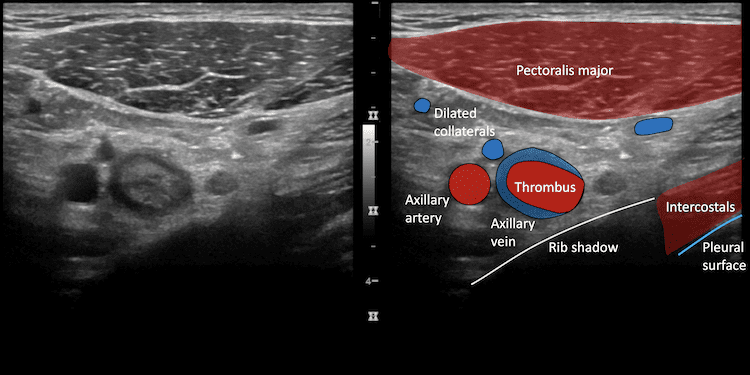
Image 4: Longitudinal view of the axillary vein
Demonstrating slow flow – known as spontaneous echo contrast or smoke. Extremely slowly moving blood is even more echogenic and is seen in the vessel behind one of the valves.
Image 5: Longitudinal axillary and subclavian vein showing intraluminal thrombus.
Image 6: Longitudinal view of the subclavian vein, supraclavicular approach, with flow demonstrated at the junction with the internal jugular vein.

CLINICAL CORRELATION
Upper limb DVT – Paget-Schroetter syndrome
Paget-Schroetter syndrome or effort thrombosis is axillary-subclavian vein thrombosis associated with repetitive use of the upper limb. Repetitive micro-trauma often accompanied by anatomical abnormalities of the thoracic outlet lead to two of the three entities of Virchow’s triad – endothelial injury and slow flow – ultimately leading to venous thrombosis. Predisposing anatomical abnormalities can include a cervical rib, congenital bands, hypertrophy of scalenus tendons and abnormal insertion of the costoclavicular ligament. The narrow path the subclavian vein must traverse through the costoclavicular space also slows flow and restricts mobility of the vein making it more susceptible to trauma with repetitive use.
Extensive subclavian and axillary venous thrombosis is relatively easy to detect, but it is easy to miss a small section of thrombus sitting just at the junciton of the subclavian and internal jugular, often deep to the clavicle. Rather than direct visualisation, Doppler assessment of flow patterns comparing the subclavian and axillary veins bilaterally can demonstrate poor emptying on the symptomatic side with reduced respiratory variation. CT venogram on standard venogram can more reliably demonstrate isolated and proximal subclavian thrombus.
Management is controversial and should involve vascular surgery and interventional radiology who will consider targeted thrombolysis and surgical intervention depending on the case.
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |