
![]()
John Thomas sign
The John Thomas sign (JT sign) is also known as Throckmorton sign is observed radiographically in male patients. A patient has a positive JT sign if his penis points towards the side of pathology on a radiograph of the pelvis.
The sign tends to be commented on by middle-aged male radiologists and orthopedists suffering from Peter Pan syndrome. Some may even suspect an occult fracture purely based on the observed radiographic penile orientation. While this can clearly be very amusing (in the same way that some people can’t help but laugh when they hear the word “Uranus”) the question remains – is the sign actually of any use?

A few studies have tried to answer this question.
1998 – The first was published by a few of my countrymen in the Medical Journal of Australia. They found that the the sensitivity (70%; 95%CI 62-78%) and specificity (67%; 95%CI 60-75%) for the JT sign were low.
2007 – Ya’ish and Baloch found that JT sign had sensitivity of 30.0% (95% CI 21.2-40.0%) and specificity of 86.0% (95%CI 77.6 – 92.1%).
2010 – Saeed Solooki and Amir Reza Vosoughi reviewed the usefulness of the John Thomas sign in determination of lower limb fractures. They evaluated 500 plain pelvic radiographs of male patients with single fracture in the lower limb. Positive sign was defined as direction of the penis shadow to the fractured limb. They found the sign to be positive in 87.8% of cases. Strongest positive correlation in patients with hip fractures.
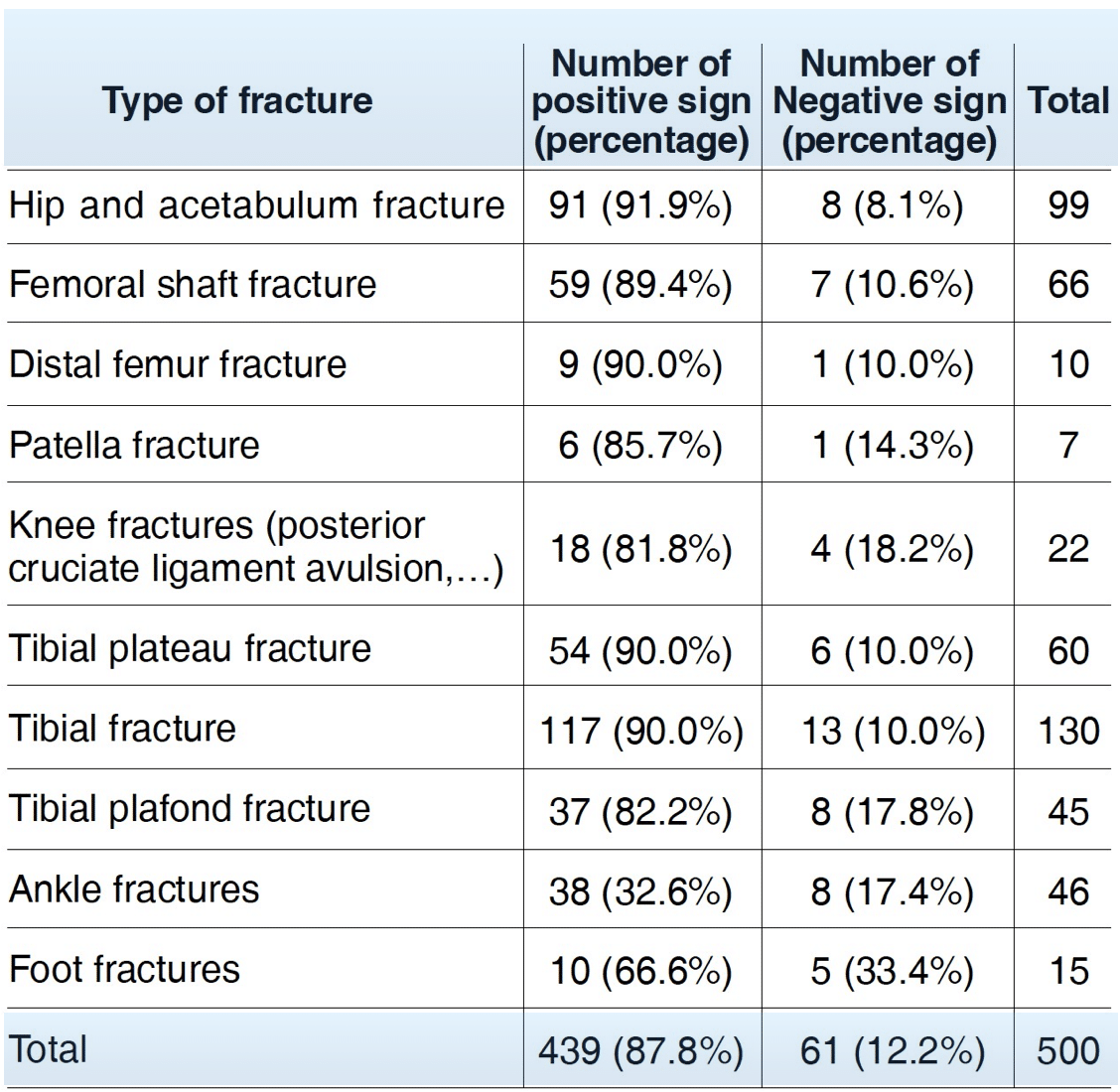
Number (Percentage) of positive and negative JT sign in each fracture group. Solooki et al 2010
2014 – Murphy et al evaluated the accuracy of the JT sign in the context of a consecutive series of male patients with hip fractures and tried to determine a relationship between side/size of penile lie and the side of fracture. They observed 200 male AP pelvis radiographs; 100 with hip fracture and 100 as control. The patient age as well as side, length and angle of penile lie were measured. They found the JT sign was positive in 46 cases, neutral in 11 and negative in 43 cases and found no link between side of fracture and penile attitude.
2019 – Gerber et al assessed the clinical validity and accuracy of the JT sign (JTS) by performing a systematic review and meta-analysis. Nine articles were isolated and assessed and 6 were analyzed further. The JTS was positive in 1089 out of 1439 patients with a pooled sensitivity of 75.7% (95%CI, 73.4%-77.9%). There was a large variation in the sensitivity and specificity amongst studies, accounting for a non-significant summary. Odds Ratio effect of -0.03. They concluded that the penile shadow on an AP pelvic X ray is not a reliable “pointer” in determining the laterality of a pelvic or hip fracture.
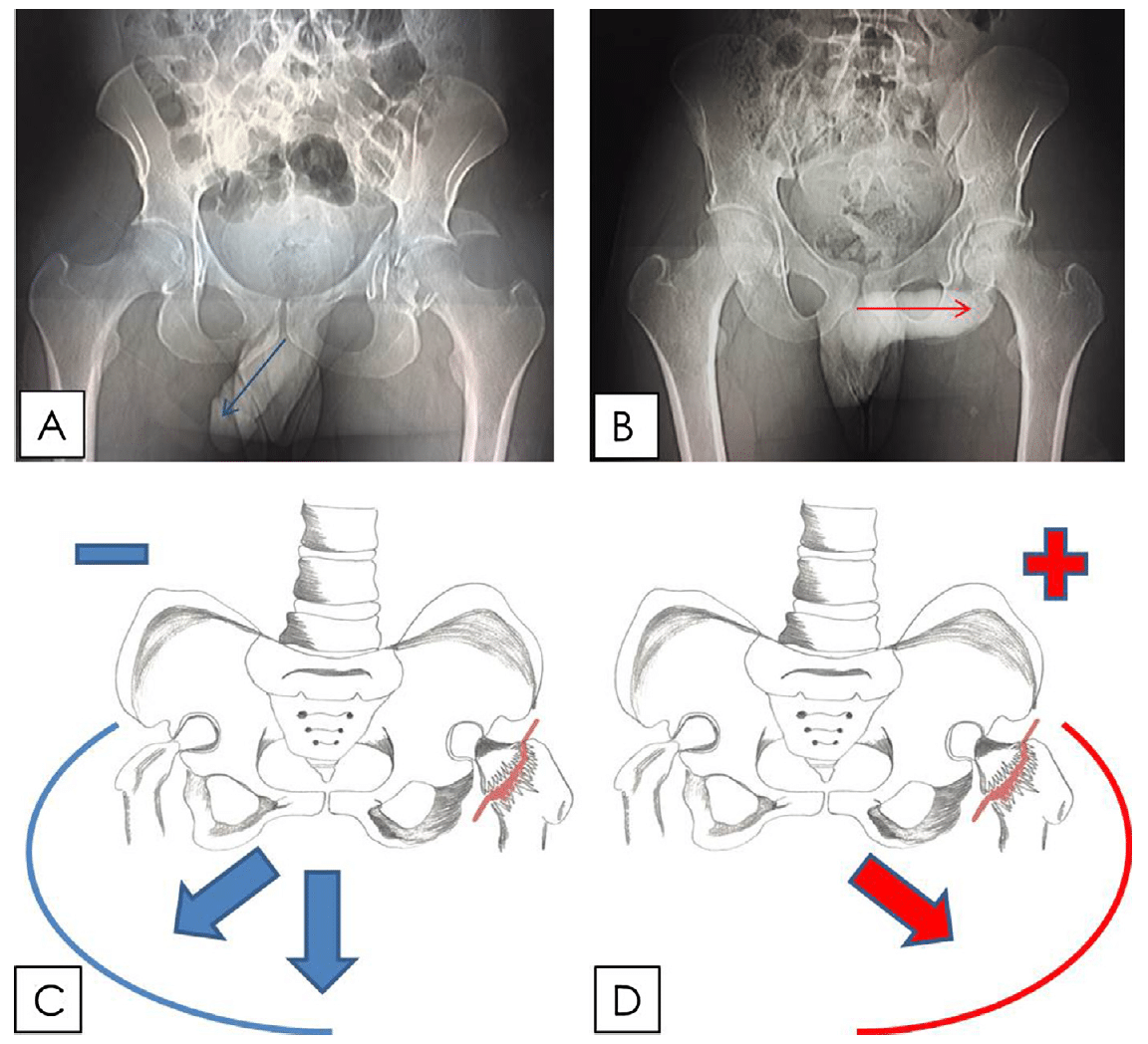
Fig. 3. Illustration of the Positive and Negative JTS (John Thomas Sign). Gerber et al 2019
3a. Negative JT sign, penile shadow points away from left acetabular fracture
3b. Positive JT sign, penile shadow points towards the left acetabular fracture.
3c. Negative JT sign, penile shadow (arrows) is neutral or points away from the side of the fracture (left neck of femur fracture).
3d. Positive JT sign, penile shadow (arrows) points towards the side of the fracture (left neck of femur fracture)
Clearly there are significant disparities in the findings of these studies, and a larger study is urgently needed. A future study must control for confounders such as patient handedness, whether boxers or briefs are worn, and which way things usually like to hang.
At this stage, although JT sign compares reasonably well with Homans sign (a useless test some misguided souls might still use to diagnose deep vein thrombosis), I think the astute emergency physicians among us will wisely elect to actually look for pathology on the radiograph rather than rely solely on the JT sign.
Conclusion: more studies needed.
References
- Thomas MC, Lyons BD, Walker RJ. John Thomas sign: common distraction or useful pointer? Med J Aust. 1998 Dec 7-21;169(11-12):670
- Ya’ish F, Baloch K. John Thomas Sign: Truth or Myth?. The Internet Journal of Orthopedic Surgery. 2007; 8(2).
- Mouzopoulos GJ, Stamatakos MK, Mouzopoulos DJ. Does penis radiological shadow indicate the side of hip fracture? J Postgrad Med. 2007; 53: 217-218
- Brink O, Borris LC, Andersen K, Hougaard K. Orams tegn på hofte- eller baekkenlidelse [Oram’s sign for hip or pelvic disorder]. Ugeskr Laeger. 2009 Dec 14;171(51):3760-3. Danish.
- Solooki S, Vosoughi AR. John Thomas sign: is it helpful to determine the lower limb fracture? Pakistan J Radiol. 2010; 20: 134-135
- Mcneillis B, Wigley J, Shantikumar S. Can John Thomas help identify hip fractures? A retrospective study and combined analysis. QJM An Int J Med Oxford. 2011;104:354
- Murphy IG, Murphy CG, Heffernan EJ. John Thomas sign–a memorable but misleading sign in hip fractures. Orthop Traumatol Surg Res. 2014 Apr;100(2):199-202
- Jeys LM. Yorkshire men straight to the point, or not? Validation of the John Thomas Sign. BMJ 2000; 321: 1609
- Gerber L et al. The ‘John Thomas’ sign and pelvic fractures-Fact or humorous myth?: A systematic review and meta-analysis. J Clin Orthop Trauma. 2019 Jan-Feb;10(1):161-166
- Foley R. Throckmorton sign (pelvis). Radiopaedia
- Cadogan M. Tom Bentley Throckmorton (1885-1961). LITFL
- Cadogan M. Throckmorton sign. Eponym A Day, Instagram

[cite]
eponymictionary
the names behind the name
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
