
![]()
Joseph O’Dwyer

Joseph O’Dwyer (1841 – 1898) was an American physician
Described as the “father of laryngeal intubation in croup.” A modest and compassionate man, O’Dwyer devoted much of his life to battling laryngeal diphtheria among children in the New York Foundling Asylum.
Despite many failures and criticisms from the medical society, O’Dwyers’ dogged tenacity in his studies saw him pioneer many a method from which the groundwork of modern intensive care is built upon today.
O’Dwyer was also one of the earlier physicians to advocate for and recognise the value of the diphtheria anti-toxin. His other achievements include the introduction and development of the O’Dwyer plain tube and a system for intralaryngeal intubation and treatment of chronic laryngeal stenosis in adults and diphtheritic asphyxia in children. He developed an apparatus for ‘artificial respiration’ in collaboration with Dr Fell known as the Fell-O’Dwyer apparatus
Biography
- Born on October 12, 1841 in Cleveland Ohio
- 1866 – graduated from College of Physicians and Surgeons in New York and worked for next 2 years at Charity Hospital in New York as ‘sanitary superintendent.’ Transferred thereafter to general practice with D Warren Schoonover
- 1872 – appointed as medical staff for Sisters of Charity New York Foundling Asylum and dedicated much of his professional life to the care of orphans or children of the poor. His dissatisfaction with the high rates of diphtheria among children and asphyxiation by laryngeal pseudomembrane lead him to develop a system for intralaryngeal intubation and design airway tubes.
- The standard treatment at the time was tracheotomy and when asked what led to the creation of his tube O’Dwyer replied, ‘Complete failure with tracheotomy in the New York Foundling Hospital, extending over a period of several years.’
- 1880 – Initial designs were modifications of the tracheotomy tube and were unsuccessful. By 1880, O’Dwyer developed metal tubes to sit subglotally within the vestibule or a ‘channel through the larynx‘
- His first design was a bivalved spring tube where the ‘valves’ were designed to spring apart and grip the larynx after the introducer is removed. 4.4-7.6cm in length with a ‘rubber collar’ (chloroform-softened gutta percha) to prevent displacement of the tube down the larynx
- 1882 – joined by Willian Perry Northrup (1851–1935) as research co-worker. First intubation with a laryngeal spring/speculum developed by O’Dwyer occurs in a conscious 4yo child with diphtheria. This relieves her asphyxia however on removal of the laryngeal spring, she relapses and a tracheostomy is performed instead. The child shortly dies thereafter as such, O’Dwyer does not count this as his first successful intubation
- 1883 – performs the third documented intubation under chloroform anaesthesia. Extubation occurs almost immediately to allow for extraction of the wide pseudomembrane intruding upon the tube and occluding the airway. Re-intubation is re-attempted however 5 hours later when the child was extubated, her condition worsened and she dies. O’Dwyer abandons the spring design of his tubes and begins work on a new tube ‘a [solid] tube of plain oval form‘
- 1884 – April; the first intubation with the new plain tube is performed on a 2 month old child. This relieves the asphyxia however the child dies 16hrs later from presumed diphtheria toxicity. The second intubation follows in May. The child is intubated for 67hours, re-intubated shortly after extubation for relapse and 7 days later ‘coughs’ out the tube. She is the first successful intubated patient who survives with use of O’Dwyers plain tube.
- Unfortunately, the next 7 intubations that follow are unsuccessful; O’Dwyer continues to make alterations to his designs to address problems such as ulceration, feeding and tracheal casts of the membrane
- 1885 – first intubation for an adult patient with laryngeal stenosis; goes on to treat other similar patients and develops his first adult tube set. In one case, he intubates the lady 8 times over 18 days with progressively increasing tube size and lengthening periods between insertions such that in 1894, he is able to report (at Bristol, UK) a freedom from restenosis that lasted 5 years
- 1885-1886 O’Dwyer performs a total of 50 intubations in private practice; 12 of which survive and an average intubation period of 5.3 days. O’Dwyer publishes two major case series of 50patients in 1887 and 1888
- 1891 – modifies George Fell (1849-1918) method of delivering artificial respiration by using his own airway tubes in place of Fells’ face mask or tracheotomy tube; introduces the design to paediatricians in Washington although the first depiction of what is later known as the Fell-O’Dwyer apparatus doesn’t appear until a paper titled “Two cases of morphine-poisoning treated principally by forced respiration” by James Voorhees in 1895
- 1894 – presents his methods of intubation at the 62nd Annual Meeting of the British Medical Association in Bristol; he is the first to develop a systematic method for intubation with successful use on enough patients to establish its validity in saving lives
- 1896 – presents a detailed history of ‘The evolution of intubation‘ at the 8th Annual Meeting of the American Paediatric Society; Northrup publishes on the clinical application of the Fell-O’Dwyer apparatus. O’Dwyer serves as president of the American Paediatric Society
- Dedicates his latter years to the study of pneumonia; dies from stroke and secondary meningitis on January 7, 1898
Medical Eponyms
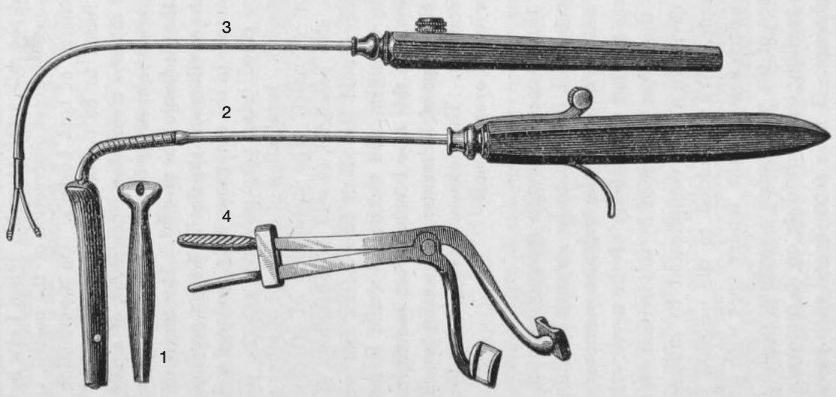
The Fell-O’Dwyer apparatus [O’Dwyer-Fell apparatus]
Consisted of a metallic right-angular curved oral tube comprised of a conical head distally and two ports proximally. Gas flow was passed through one port from a Fell system of bellows and a rubber delivery tube and expired air vented from the second port. The second port could be occluded intermittently by the operators thumb thus acting as a ‘valve’ and enabling IPPV.
…some wonderful results in cases of respiratory failure have been accomplished with this apparatus.
…a male ward patient suddenly stopped breathing; Dr David Bovaird, an intern at that time had an O’Dwyer-Fell apparatus handy. He got this going and the patient’s pulse came back…artificial respiration was continued for a couple of hours…it was then stopped…pulse again began to fade…artificial respiration was then resumed with a return of the heart’s action….life was kept in this patient twenty four hours…realising the hopelessness of this case, discontinued artificial respiration and the patient promptly died….
I have quoted this case to show the possibilities of this form of artificial respiration
O’Dwyer. Medical Record, 1911
The Fell-O’Dwyer apparatus underwent several modifications over time.
The apparatus was introduced to Charity Hospital in New Orleans by surgeon Dr J.D. Bloom who adapted the apparatus (Fig c.) for use for pulmonary insufflation in asphyxia neonatorum. His modification is described in a paper on ‘Intralaryngeal Insufflation’ by vascular surgeon Rudolph Matas (1860-1957) in 1900:
Dr Bloom has found it advantageous to modify the accessory or inflating part of the apparatus by several additions which deserve mention, as they save unnecessary exertion on the part of the operator and diminish the strain on the bellows…“a long lever (…) used as a treadle to compress the bellows with the foot…a metallic cylinder which is fitted with absorbent cotton to filter the air as it passes from the bellows to the patient
Matas 1900
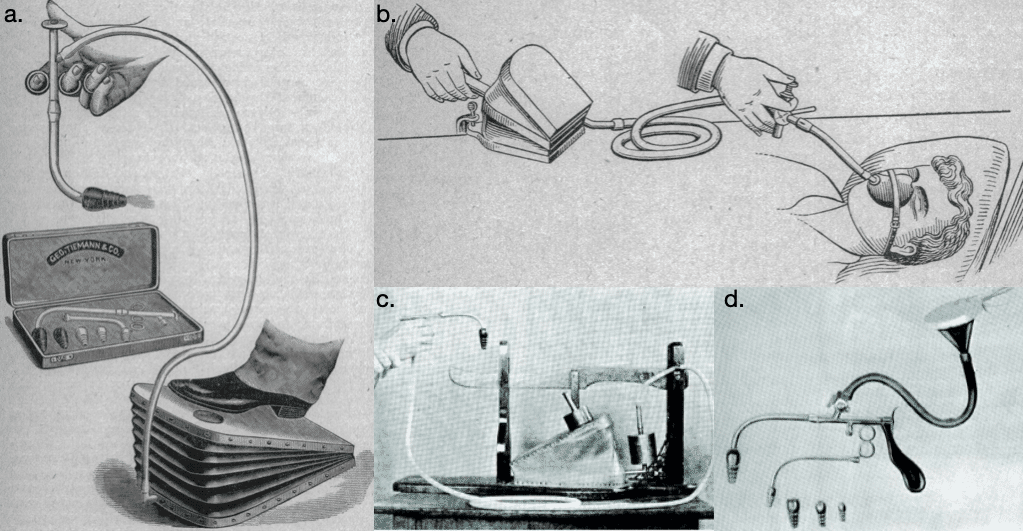
b. Fell apparatus for artificial respiration (1900);
c. J. D. Bloom’s modification of the Fell-O’Dwyer apparatus (1900);
d. Matas modification of O’Dwyer’s intubating apparatus (1900);
A tube could also be attached to an oxygen source to provide oxygenation during cases of asphyxia.
Dr Matas’ modification of the Fell-O’Dwyer apparatus (adapted for his use for intrathoracic surgery, see Fig d.) included the addition of a cone with a stop cock that controlled the supply of anaesthetic gases without “interfering with the passage of air furnished by the bellows or air pump.” A pistol shaped handle was also designed to allow for easier control.
I have also modified the apparatus so that it is provided with one aspirating as well as insufflating valve. While the aspirating valve is rarely used, it may occasionally find application in cases of excessive clogging of the larynx with mucus, food, foreign matter and other substances that may threaten life by their presence…the aspirating valve may be utilized to insufflate oxygen pure or mixed with atmospheric air
Matas 1900
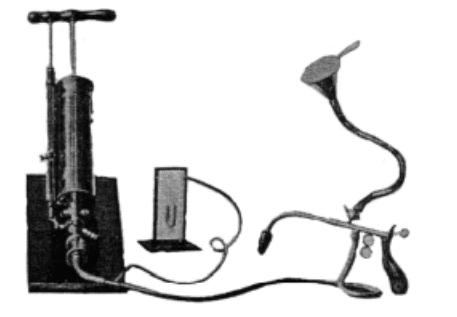
in 1902, Matas collaborated with engineer and surgeon Dr John Smythe to further modify the apparatus. It now included a single graduated cylinder to enable delivery of precise volumes of air up to 1, 500cm3, a mercury manometer for measurement of intrapulmonary pressure and a modified Fell-O’Dwyer intralaryngeal cannula to include a port for delivery of anaesthetic or oxygen during artificial respiration
The innovations of O’Dwyer gradually fell from favour.
The preference for continuous intratracheal insufflation by US anaesthetists, introduced in 1907 by Barthelemy et Dufou (de Nancy) saw the Fell-O’Dwyer apparatus fall out of use and the emergence of more novel forms of artificial respiration.
O’Dwyer tubes which had largely replaced tracheotomy by 1895, declined in use thereafter with the development of anti-toxins for diphtheria which saw a falling need for intubation.
O’Dwyer was among the first to recognise the value for diphtheria anti-toxin, an innovation of Pierre-Paul Emile Roux of Paris, which in its early stages was largely repudiated by the medical community. O’Dwyer’s persistence inevitably lessened the need for intubation. His tubes were eventually superseded during the 1920’s, with the advent of the single lumen endotracheal tube by Ivan Magill and Stanley Rowbotham which became the dominant form for anaesthesia
Criticisms
Intubation is O’Dwyer’s monument. It is equally true that it killed him.
Obituary O’Dwyer, BMJ 1898
Aptly described by Northup, O’Dwyer’s career and medical innovations were not without problems. Despite his numerous failures during the development of his methods, O’Dwyer was tenacious in his studies and his desire to alleviate the suffering in children with diphtheria drove him onwards. O’Dwyer however faced heavy criticism from colleagues at the asylum where he worked and the professional community who were opposed to his new methods of treatment and viewed his insertion of tubes as torturing children already suffering from severe asphyxia disease. Practitioners who did attempt O’Dwyer’s method were unskilled and unsuccessful intubations were reflected back onto O’Dwyer. In fact, he remarked:
…intubation is apparently, but not really, a simple operation
O’Dwyer 1894
To add insult to injury, O’Dwyer did not patent his tubes thus all manner of cheap imitation tubes were available in America and Europe and brought with them all the problems that O’Dwyer had spent much of his life work circumnavigating.
Major Publications
- O’Dwyer J. Intubation of the larynx. New York Medical Journal 1885; 42: 145-147.
- O’Dwyer J. Feeding after intubation of the larynx. With exhibition of tubes modified to overcome difficulties in feeding. Medical record (New York) 1887; 31: 685-686.
- O’Dwyer J. Fifty cases of croup in private practice treated by intubation of the larynx, with a description of method and of the dangers incident thereto. Medical record (New York) 1887; 32(18): 557-61
- Jacobi A, O’Dwyer J, Huber F, Brown D, Northrup WP, Hance IH, Caille A. Intubation of larynx : papers read before the New York Academy of Medicine, in the stated meeting of June 2, 1887. Medical Record reprint 1887
- O’Dwyer J. Analysis of fifty [further] cases of croup treated by intubation of the larynx. New York Medical Journal. 1888; 47: 33-37.
- O’Dwyer J. An improved method of performing artificial forcible respiration (with exhibition of instruments). Archives of pediatrics 1892; 9: 30-34.
- O’Dwyer J. Intubation in the treatment of chronic stenosis of the larynx. II. Br Med J 1894; 2: 1478-1481
- O’Dwyer J. The evolution of intubation. Transactions of the American Pediatric Society 1896; 8: 9-20.
- O’Dwyer J. The evolution of intubation [without figure] Archives of pediatrics 1896; 13(6): 401-413
- O’Dwyer J. The O’Dwyer forcible respiration apparatus for children. Medical record (New York) 1911: 80(12): 576-577
Intubation…was perfected through the conscientious labors of the self-sacrificing Joseph O’Dwyer whose name stands with those of Semmelweis and Crede as the greatest benefactor of infant life.
Fielding Hudson Garrison (1913)
References
Biography
- Obituary: Joseph O’Dwyer MD. Br Med J 1898; 1: 594
- Walsh JJ. Biographical notes on Joseph O’Dwyer, MD. 1841-1898. The inventor of intubation. Records of the American Catholic Historical Society of Philadelphia. 1903; 14(4): 391-422
- Garrison GH. An introduction to the history of medicine. 1914: 554
- Ruhräh J. Joseph O’Dwyer 1841-1898. Note on the history of intubation. Am J Dis Child. 1935; 50(4): 998-1002
- Walsh JJ. Dr. Joseph O’Dwyer, Inventor of Intubation. Linacre Quarterly. 1939; 7(2): 43-44
- Trubuhovich RV. 19th century pioneers of intensive therapy in North America. Part 2: Joseph O’Dwyer. Crit Care Resusc. 2008 Jun;10(2):154-68
- Wiedemann HR. Joseph O’Dwyer (1841-1898). Eur J Pediatr. 1992 Jul;151(7):471.
Eponymous terms
- Voorhees J. Two cases of morphine-poisoning treated principally by forced respiration. Medical record (New York) 1895; 48(21): 768-769
- Northrup WP. Apparatus for artificial forcible respiration. Medical and Surgical Reports of the Presbyterian Hospital 1896; 1: 132
- Matas R. Intralaryngeal insufflation: for the relief of acute surgical pneumothorax. Its history and methods with a description of the latest devices for this purpose. JAMA. 1900; XXXIV(22): 1371-1375 and JAMA. 1900; XXXIV(23):1468-1473
- Trubuhovich RV. 19th century pioneering of intensive therapy in North America. Part 3: the Fell-O’Dwyer apparatus and William P Northrup. Crit Care Resusc. 2009 Mar;11(1):78-86.
Eponym
the person behind the name

FACEM. Emergency physician and researcher at Sir Charles Gairdner Hospital, Perth
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |