
![]()
George Fell

George Edward Fell (1849–1918) was an American surgeon, engineer and inventor
Fell was the innovator of ‘forced respiration’ better known as IPPV, a method he developed in anaesthetised dogs and later adapted for human use. He found its applications in patients with opiate overdoses and advocated for its broader use in other life-threatening conditions including traumatic shock, asphyxia and thoracic surgery.
Unfortunately, Fell was met with great resistance from the medical community and the Fell method of respiration never reached widespread uptake into practice. Instead, he spent much of his career tenaciously campaigning for its use and seeking recognition for his efforts.
The Fell apparatus however, did eventually rise to prominence to outlive its inventor by the efforts of John O’Dwyer (1841-1898) and Rudolph Matas (1860-1957) who introduced modifications giving the apparatus a more established presence in the medical world.
On an interesting side note, Fell was involved in the final design of the electric chair, an endeavour that he felt enabled a more “humane execution,” a humorous paradox to the medical professional he was.
Biography
- Born on July 10, 1849 in in Chippewa, Ontario
- 1869 – completes engineering studies, University of Buffalo and begins working as a Buffalo city engineer
- 1879 – founding member of the American Society of Microscopists; works as assistant engineer on Ontario-New York State International Bridge whilst concurrently studying medicine
- Paradoxically, works on the design and creates the first electric chair; he conducts a series of studies in dogs on the effects and methods of electrocution. Despite being against Capital punishment, views his work as means to create a more ‘humane’ method of execution
- 1882 – MD, University of Buffalo defends thesis on the ‘Histology of aneurismal clots‘
- 1884 – Chair of Physiology and Microscopy at Niagara University; studies and develops methods for applying IPPV with household bellows through a tracheotomy in anaesthetised dogs. Remarks that “if the respirations could be kept up by suitable means for a sufficient time to permit the elimination of the poison, life may be saved…”
- 1886 – Witnesses the attempted resuscitation of a man with morphine overdose, resolves to better the methods for artificial respiration
Electricity, atropia, coffee extract, brandy and active movements were used. Artificial respiration, by “Sylvester’s” method, was also employed…but the patient soon succumbed to the inevitable. At this time, I felt keenly the inadequacy of the methods at our command, and then resolved, if opportunity ever offered, to make the operation which I have now to record and which, I believe, might have saved Mr. Dyke’s life.
Fell 1887
- 1887 – Fell’s first successful case using ‘forced respiration” (IPPV) on an alcoholic man with opium poisoning occurs on July 23. He describes the case in his article ‘Forced respiration in opium poisoning – its possibilities, and the apparatus best adapted to produce it’ in the Buffalo Medical Surgical Journal.
- The second case follows shortly on December 10, in a patient with laudanum poisoning and forced respiration is given for 14.5hours. Fell suggests the need for electromotive power in place of manual labour for future cases (although this does not eventuate in his time). He continues to apply the ‘Fell method’ to over 30 patients and keeps meticulous documentation of each.
- 1893 – presents a 28-plus case series at the Pan-American Medical Congress, again to poor reception. Publishes multiple cases histories of successful forced respiration over the next 8 years in journals such as Buffalo Medical Journal, Archives of Paediatrics, Canada Medical record and the Medical Examiner.
- 1896 – publishes a case report titled ‘The value of forced artificial respiration (Fell method) in saving human life in chloroform, ether, and nitrous-oxide narcosis, together with the account of a remarkable case in which it was used for four days and three nights upon a physician, resulting in saving his life’
- Fell describes a case of successful forced respiration in physician Dr Henry Williams who required 80 hours of ventilation for opiate overdose. Following this case, Fell received strong medical support and the value of his work is recognised; he begins to advocate for other potential uses of his method in particular to thoracic surgery, an idea later taken up by vascular surgeon Rudolph Matas(1860-1957)
- 1899 – publishes article ‘Remarkable cases of life saving by the Fell method of forced artificial respiration‘
- Does not appear in medical literature again until 1910 with two further articles; remains a strong advocate (if not aggressive) for forced respiration.
- In the last 6 years prior to his death, little is known about the events surrounding Fell.
- He died on July 29, 1918
Medical Eponyms
Fell’s apparatus
Fell’s initial apparatus was developed from his experiments in anaesthetised dogs and comprised a foot bellow connected via rubber tubing to a ‘one piece’ unit which included a directional control valve and a tracheotomy tube. The stop cock on the valve had to be manually turned by hand for each inspiration and expiration.

Following his landmark case in 1888, Fell modified the design of his apparatus to adapt it better to human use. The bellows were equipped with a rubber equaliser to enable smoother and more rhythmical delivery of air; the control valve was swapped for a two-way valve which could be controlled by the operators’ fingertip to deliver IPPV as needed. The tubing was changed to a more flexible one and inserted between the valve and tracheotomy tube. This prevented tugging on the trachea from the turning of the stop cock, a problem with the original design.
He who would attempt to save human life by forced respiration must be supplied beforehand with suitable apparatus
Fell, 1889
The apparatus could also be used to deliver IPPV with a face mask rather than tracheotomy and whilst Fell did successfully manage some patients with this method, he was faced with the complication of gastric insufflation and aspiration.
For physicians who were reluctant to perform a tracheotomy, the option for face mask and IPPV made Fell’s method more attractive as well as encouraged its use. It could also ‘buy time’ for the moribund patient to relieve the acute crisis so that a tracheotomy could then be performed safely. However, control for the rate of respiration was quite strenuous on the operator (or so it appears) with Fell noting that “…bellows working at the rate of 108 movements per minute, patient by this means receiving 21 respirations to the minute” [Case V, 1888].
Perhaps most prominent of the modifications to this apparatus, were the additions made by Joseph O’Dwyer (1841 – 1898) who replaced Fell’s tracheotomy with his own laryngeal tubes thus introducing the ‘Fell-O’Dwyer apparatus.’ Fell initially objected to intubation stating that it ‘would prevent the imbibing of fluids, through which means we may most readily aid elimination of the poison’ and that ‘the time lost in attempted intubation in drowning cases would make the operation impractical.’
Fell’s viewpoint later changed as the Fell-O’Dwyer apparatus became more established in clinical use and designed his own laryngeal tube in 1908 – a tube he felt was less injurious than that of O’Dwyer’s (although never quite gained the traction as did O’Dwyer’s tube in medical practice).
The Fell-O’Dwyer apparatus underwent several modifications over time.
The apparatus was introduced to Charity Hospital in New Orleans by surgeon Dr J.D. Bloom who adapted the apparatus (Fig c.) for use for pulmonary insufflation in asphyxia neonatorum. His modification is described in a paper on ‘Intralaryngeal Insufflation’ by vascular surgeon Rudolph Matas (1860-1957) in 1900:
Dr Bloom has found it advantageous to modify the accessory or inflating part of the apparatus by several additions which deserve mention, as they save unnecessary exertion on the part of the operator and diminish the strain on the bellows…“a long lever (…) used as a treadle to compress the bellows with the foot…a metallic cylinder which is fitted with absorbent cotton to filter the air as it passes from the bellows to the patient
Matas 1900
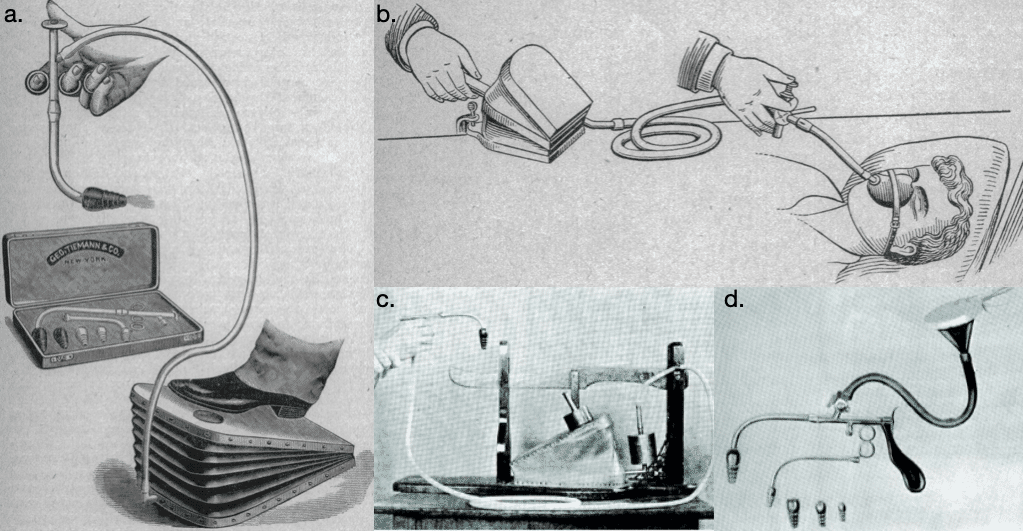
b. Fell apparatus for artificial respiration (1900);
c. J. D. Bloom’s modification of the Fell-O’Dwyer apparatus (1900);
d. Matas modification of O’Dwyer’s intubating apparatus (1900);
A tube could also be attached to an oxygen source to provide oxygenation during cases of asphyxia.
Dr Matas’ modification of the Fell-O’Dwyer apparatus (adapted for his use for intrathoracic surgery, see Fig d.) included the addition of a cone with a stop cock that controlled the supply of anaesthetic gases without “interfering with the passage of air furnished by the bellows or air pump.” A pistol shaped handle was also designed to allow for easier control.
I have also modified the apparatus so that it is provided with one aspirating as well as insufflating valve. While the aspirating valve is rarely used, it may occasionally find application in cases of excessive clogging of the larynx with mucus, food, foreign matter and other substances that may threaten life by their presence…the aspirating valve may be utilized to insufflate oxygen pure or mixed with atmospheric air
Matas 1900
Criticisms
Fell was a strong advocate of his method for forced respiration giving often opinionated remarks against other medical colleagues who he felt were not giving him due credit for his work. These included Dr Jean Baptiste Vincent Laborde and Professor Horatio Wood who had separately recommended forced respiration without acknowledging ‘Fell’s Method.’
To be denied the credit which should in all fairness be accorded to the practical originator of a method of such far-reaching importance in the saving of human life is what I could not and will not quietly submit to. “Honor, gentlemen, to whom honor is due.“
Fell, 1893: 124
Fell held particular resentment against Marshall Hall (1790-1857) whom he felt bore in part the responsibility for the medical professions’ resistance to forced respiration where “…the prevailing opinion at that time was that the air vesicles of the lungs would not resist forcible mechanical measures in artificial respiration” [Fell, 1896]
Marshall Hall indeed, considered the use of bellows as highly dangerous
But another objection applies to the mode of inducing artificial respiration having the character of the forcing-pump.…a degree of force must be used, sufficient to raise the bony and other structures of the thorax….which both anticipation and experience prove to be injurious to the delicate structure of the lungs…found these structures variously lacerated by this measure in experiments with animals
The obvious conclusion is, that, whenever we attempt artificial respiration, the procedure must be effected with gentleness and slowness
Hall M: Asphyxia, presented to the Royal Humane Society in London 1856
Fell knew that his method would be considered sinful especially to those who upheld Marshalls strictures on artificial respiration however, Fell was far from timid in his beliefs:
And thus another human life was saved, and accident, prejudice or ignorance again frustrated by a method which that great medical authority, Marshall Hall, said should never be used and the whole medical world had accepted as “Law and Gospel,” which it is a medical sin to trespass upon.
So I am a medical sinner and a bad one, for I glory in my sin, which has now saved a few hundreds of human lives and is destined to save thousands.
Fell GE, 1899
The electric chair
Electrocution, which was first suggested by Dr. AP Southwick of Buffalo, N. Y., was made practical by the investigative work of Dr. Fell. He made the vivisection experiments which resulted in his conclusion:
First – That death produced by a sufficiently powerful electrical current is the most rapid and humane produced by any agent at our command. Second – That resuscitation, after the passage of such a current through the body and functional centres of the brain, is impossible. Third – That the apparatus to be used should be arranged to permit the current to pass through the centres of function and intelligence in the brain
Fell, Obituary 1918
Major Publications
- Fell GE. Forced respiration in opium poisoning – its possibilities, and the apparatus best adapted to produce it. Buffalo medical and surgical journal. 1887; 27(4): 145-157
- Fell GE. Forced respiration – Case No. 3. Buffalo medical and surgical journal. 1888; 27(8): 345-353
- Fell GE. Forced respiration.- History. – Report of six cases; apparatus; effects of, on narcotised human subjects; adaptability of, in cases of drowning or shock. Transactions of the New York State Medical Association for 1888; 5: 36-65.
- Fell GE. Forced respiration: additional observations. Transactions of the New York State Medical Association for 1889; 6: 316-320
- Fell GE. Forced respiration. Delivered in the Section of Practice of Medicine, Materia Medica and Physiology, at the Fortieth Annual Meeting of the American Medical Association, June, 1889. JAMA. 1889; XIII(15): 519.
- Fell GE. Forced respiration: continued observations. Transactions of the New York State Medical Association for 1891; 6: 176-190
- Fell GE. Forced respiration. Answer to article of Dr J O’Dwyer on [An improved method of performing artificial forcible respiration] Archives of pediatrics 1892; 9: 342-349
- Fell GE. Additional evidences of the value of forced respiration (Fell method), in opium narcosis. Report of cases. JAMA. 1892; XIX(5):130-133
- Fell GE. Fell method – Forced respiration. Report of cases resulting in the saving of twenty-eight human lives. History and a plea for its general use in hospital and naval practice. Canada Medical Record 1894; 22: 73-88; 97-105; 121-127.
- Fell GE. The value of forced artificial respiration (Fell method) in saving human life in chloroform, ether, and nitrous-oxide narcosis, together with the account of a remarkable case in which it was used for four days and three nights upon a physician, resulting in saving his life. Medical Record (New York) 1896; 49(22): 760-763.
- Fell GE. Remarkable cases of life saving by the Fell method of forced artificial respiration. The Medical Examiner. 1899; 9(6): 168-171.
- Fell GE. Artificial respiration. Forced respiration, with comments on the cabinet methods of Sauerbruch, Meyer, and others; also a new method in thoracic surgery. Surgery, Gynecology and Obstetrics 1910; 10: 572-582.
References
Biography
- Obituary: Dr. George Edward Fell. Buffalo Medical Journal 1918; 74: 73-74.
- Obituary: George Edward Fell. JAMA 1918; 71: 485
- Fell, Edward George (1850-1918) In: American medical biographies. 1920
- Trubuhovich RV. 19th century pioneers of intensive therapy in North America. Part 1: George Edward Fell. Crit Care Resusc. 2007 Dec;9(4):377-93.
- Bibliography. Fell, George Edward. WorldCat Identities
Eponymous terms
- Murray J. Account of an apparatus for restoring the lost action of the lungs, in consequence of suspended animation from drowning, etc.; invented and communicated by John Murray, Esq. The London Journal of Arts and Sciences 1822; 3: 93-96
- Hall M. Abstract of an investigation into asphyxia: its nature, carbonic acid blood-poisoning, and its remedy, prone and postural respiration. London: Churchill. 1856
- Hall M. Prone and postural respiration in drowning and other forms of apnoea or suspended respiration. London: Churchill. 1857
- Manuel DE. Marshall Hall, F.R.S. (1790-1857); a conspectus of his life and work. Notes and Records of the Royal Society of London. 1980 Dec;35(2):135-66.
Eponym
the person behind the name

FACEM. Emergency physician and researcher at Sir Charles Gairdner Hospital, Perth
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |