
![]()
“Benign” Early Repolarization Misnomer
“Benign” Early Repolarization: A misnomer predicting idiopathic VF
(Benign) early repolarization was present in 31% of patients resuscitated after cardiac arrest due idiopathic ventricular fibrillation (VF), compared with 5% of control subjects. This pattern was present on all case subjects in whom pre-existing ECGs were available.
Haïssaguerre et al. NEJM 2008
In 2008, Haïssaguerre et al challenged the well-embedded term “benign” early repolarization by demonstrating a link between this familiar ECG pattern and idiopathic VF arrest
- Standard patterns of QRS-ST junction elevation > 1mm in inferior or lateral leads were found to be present in 31% of patients with idiopathic VF, with an odds ratio of 10.9 compared to control subjects
- Findings gave weight to previous experimental studies which had shown than BER predisposes to potential arrhythmogenicity but for which very limited supporting clinical evidence had been demonstrated
- Other smaller case studies have demonstrated an incidence of BER in patients with idiopathic VF of up to 60%
Le Syndrome de Haïssaguerre (idiopathic VF):
Diagnosis of exclusion in patients who have survived a VF episode without any identified structural or metabolic cause despite extensive diagnostic testing.
Early Repolarisation Syndrome (ERS)
ERS refers to the presence of a BER pattern in patients who have survived idiopathic VF. Given the higher incidence of idiopathic VF in patients with BER, the term may be more of an observation than a separate entity.
In 2011, Antzelevitch et al described different types of ERS that correlate to ECG regions of BER and their correlation to risk of recurrent VF
| ERS | BER pattern | VF recurrence |
| Type 1 | Lateral precordial leads | Low; prevalent among healthy male athletes |
| Type 2 | Inferior leads | Moderate |
| Type 3 | Global | High; association with VF storms |
In 2012, Junttila et al proposed a further classification of early repolarization (ER) patterns. They defined two types of J-point elevation:
- Benign form: J-point with rapidly ascending ST segment
- Malignant form: J-point with horizontal or descending ST segment
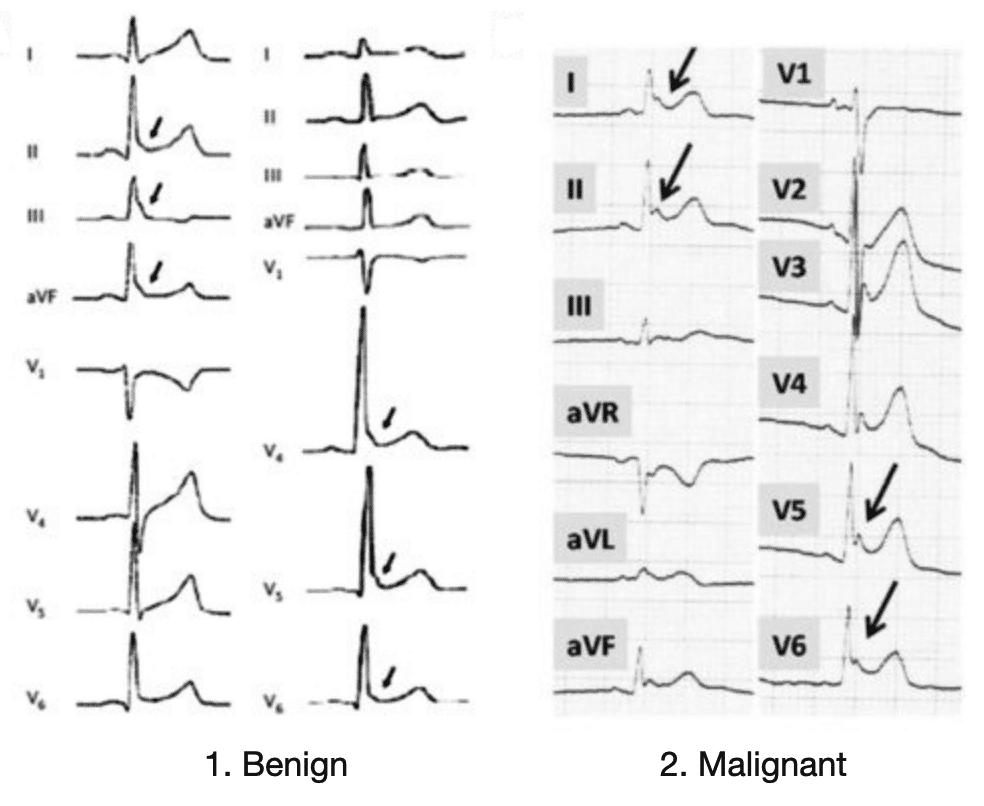
B. Malignant type with horizontal variety of ER.
Source: Sethi et al 2014
The electrophysiology
Idiopathic VF requires a triggering ectopic, usually short-coupled PVCs, and a maintenance substrate
- When identifiable, 80-90% of triggering ectopics originate from the Purkinje system or neighbouring structures (moderator band, papillary muscles)
- VF requires the continuous formation of reentry for its maintenance, often which is localised to a myocardial region with identifiable structural abnormalities (fibre arrangement, fibrosis). Idiopathic VF patients would be expected to have uniform reentries on electrode mapping, however when studied they also demonstrate clustering of reentries, indicting “microstructural” defects
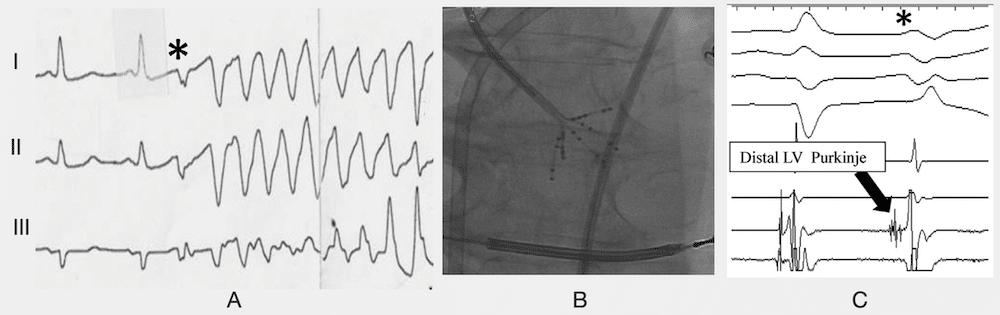
Patterns of Purkinje activity in patients with VF: Haïssaguerre 2019
(A) Typical short-coupled ectopy(*) initiating VF.
(B) Multielectrode mapping with a multispline catheter recording
(C) the earliest activity preceding ectopic beat in the distal left posterior fascicle
Clinical significance
Awareness of the correlation between BER and idiopathic VF likely lies more in preventing and treating recurrent episodes of VF, as follow up of case subjects found a higher incidence of recurrent VF. Although ICD is the treatment of choice, additional drugs may be required to prevent recurrent episodes and treat VF storms. Follow-up of patients with idiopathic VF found isoproterenol infusion the only drug reliable in treatment of VF storms, and quinidine of most benefit in preventing recurrence.
Size of J-point elevation on initial ECG displayed correlation with the number of recurrent VF episodes, with greater than 50 recurrent episodes in the three subjects with the highest J-point elevation (> 5mm). Despite this, given the prevalence of the BER pattern in the wider community, current recommendations remain that asymptomatic patients with J waves not undergo further testing.
Limitations
Subsequent studies affirming findings by Haïssaguerre et al have involved smaller patient populations, and although they confirm the link between BER and idiopathic VF, they do not allow us to discern which patients with ECG findings of BER are at risk of an initial episode of idiopathic VF. The benign natural history for most patients with BER and its prevalence among young individuals suggests other specific ECG markers are required to determine which patients would benefit from electrophysiological testing. This may include further research into types of ERS, in particular type 3 ERS with a global BER pattern, and its correlation to idiopathic VF.
Alternative names
- Haissaguerre syndrome
References
Further reading
- Burns E. Ventricular Fibrillation (VF). ECG Library
Historical references
- Haïssaguerre M et al. Mapping and ablation of idiopathic ventricular fibrillation. Circulation. 2002; 106(8): 962-967.
- Haïssaguerre M, et al. Sudden cardiac arrest associated with early repolarization. N Engl J Med. 2008 May 8;358(19):2016-23.
Eponymous term review
- Viskin S. Idiopathic ventricular fibrillation “Le Syndrome d’Haïssaguerre” and the fear of J waves. J Am Coll Cardiol. 2009; 53(7): 620-622.
- Antzelevitch C, Yan GX, Viskin S. Rationale for the use of the terms J-wave syndromes and early repolarization. J Am Coll Cardiol. 2011 Apr 12;57(15):1587-90
- Junttila MJ, Sager SJ, Tikkanen JT, Anttonen O, Huikuri HV, Myerburg RJ. Clinical significance of variants of J-points and J-waves: early repolarization patterns and risk. Eur Heart J. 2012 Nov;33(21):2639-43
- Sethi KK, Sethi K, Chutani SK. Early repolarisation and J wave syndromes. Indian Heart J. 2014 Jul-Aug;66(4):443-52
- Visser M, van der Heijden JF, Doevendans PA, Loh P, Wilde AA, Hassink RJ. Idiopathic Ventricular Fibrillation: The Struggle for Definition, Diagnosis, and Follow-Up. Circ Arrhythm Electrophysiol. 2016; 9(5): e003817.
- Hanboly NH. Haissaguerre syndrome: The gray area still exists. Nig J Cardiol 2017;14:59-64
- Cheniti G et al. Mapping and Ablation of Idiopathic Ventricular Fibrillation. Front Cardiovasc Med. 2018 Sep 18;5:123
- Haïssaguerre M et al. The Spectrum of Idiopathic Ventricular Fibrillation and J-Wave Syndromes: Novel Mapping Insights. Card Electrophysiol Clin. 2019; 11(4): 699-709
eponymictionary
the names behind the name

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
