![]()
Lover not a fighter
aka Bone and Joint Bamboozler 010
A distinctly uncommunicative 32 year-old man presents to the emergency department with a painful and swollen right hand. He said he tripped at work, broke his fall with his hand, and that its been sore since.
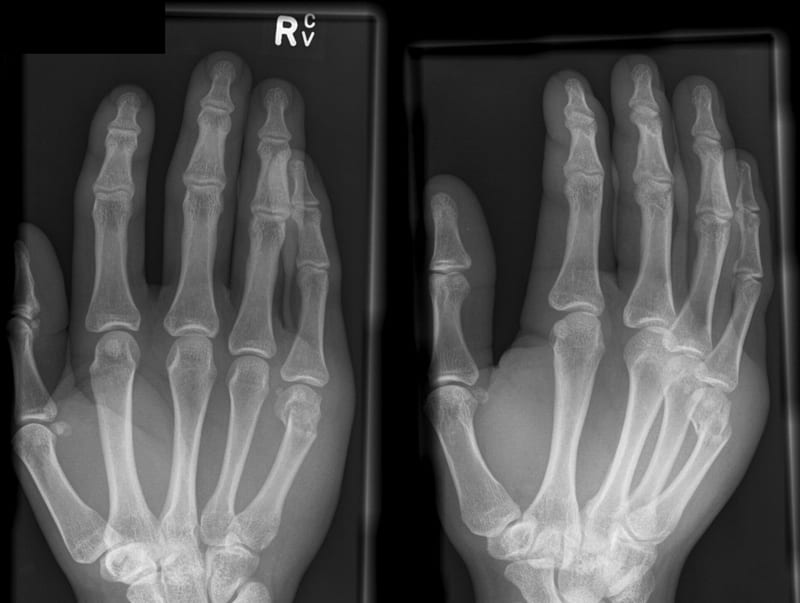
These are the radiographic images of his right hand:
Questions
Q1. Describe the injury?
Answer and interpretation
There is a fracture of the right 5th metacarpal neck.
The distal fragment is volarly displaced and angulated.
Q2. What is the eponymous name for this fracture?
Answer and interpretation
Boxer’s fracture.
A Boxer’s fracture is a metacarpal neck fracture affecting the 5th metacarpal.
The name is ironic because someone who knows how to punch will avoid focusing the impact of a blow on the knuckle of his or her little finger. Perhaps it should be renamed the ‘I’m a lover, not a fighter, fracture’?
Assume any wound associated with a Boxer’s fracture is a ‘fight bite’.
Q3. What the typical mechanism of injury?
Answer and interpretation
Metacarpal neck fractures result from direct impact on the metacarpal head with the MCP joint in flexion. This generally occurs when the patient’s fist strikes a solid object like a wall or someone else’s head…
Q4. What imaging and views are best for this assessing this injury?
Answer and interpretation
AP, lateral and oblique views should be obtained to accurate define metacarpal neck fractures, and the degree of displacement and angulation.
In this case, the true lateral is missing — this is an important view as it provides the most accurate assessment of angulation.
Q5. What specific complications can occur with metacarpal neck fractures?
Answer and interpretation
Complications can be debilitating:
- Collateral ligament damage.
- Extensor tendon injuries.
- Rotational deformity leads to finger overlap and impaired function.
- Dorsal bony prominence with compromise of the extensor mechanism.
- Clawing of the finger may occur if the reduction is incomplete or unstable.
- Chronic pain with grasp.
- Nonunion is rare.
Q6. what is an acceptable degree of deformity in different types of metacarpal neck fractures?
Answer and interpretation
Any rotational deformity in a metacarpal neck or shaft fracture should be corrected as it is poorly tolerated. This can be assessed by getting the patient to make a fist — rotational deformity will cause the fingers to cross.
Flexion deformities are more common, and better tolerated. A simple rule of thumb for the amount of volar angulation tolerate is:
- 10 degrees for the 2nd metacarpal.
- 20 degrees for the 3rd metacarpal.
- 30 degrees for the 4th metacarpal.
- 40 degrees for the 5th metacarpal.
Simon et al (2007) suggests reduction for deformities 10 degrees less than those detailed above for 3rd/4th/5th metacarpal neck fractures. Rosen’s says 15-15-35-45!
Note that the 5th MC neck normally has a volar angulation of 15 degrees — the above allowances are in addition to this.
The 5th CMC joint is much more mobile — like the thumb — so a greater degree of flexion deformity is functionally acceptable (similarly ~40 degree flexion is acceptable for 1st metacarpal fractures).
Q7. Describe the management of different types of metacarpal neck fractures?
Answer and interpretation
Metacarpal neck fractures are inherently unstable.
Management of 4th and 5th metacarpal neck fractures:
- Nondisplaced, nonangulated
- RICE
- Immobilisation with a volar splint to the palmar crease and a dorsal splint extending to, but not including, the PIP. Wrist in 30 degrees extension and MCPJ flexed to 90 degrees.
- Begin PIP and DIP movements immediately, protected MCP movements after 3-4 weeks.
- Displaced, angulated
- Reduction may be performed under a hematoma block, wrist block or even procedural sedation.
- After disimpacting the fracture, the MCPJ and PIPJ is flexed to 90 degrees (‘the 90-90 method’) — this tightens the collateral ligaments that connect the PIP to the MC head. A volar force is applied over the shaft proximal to the fracture line at the same time as a dorsally directed forced applied to the flexed PIP.
- Immobilise as for the nondisplaced/ nonangulated fracture +/- an ulnar gutter splint.
Close follow up is required as reductions are unstable and pin fixation is usually necessary.
Management of 2nd and 3rd metacarpal neck fractures:
- Nondisplaced, nonangulated
- RICE
- Immobilization in a radial gutter splint extending from the distal elbow just proximal to the PIP joint. The wrist should be in 20 degrees extension and the MCPJ should be in 50-60 degrees flexion.
- Close follow-up to detect angulation or rotational malalignment is crucial as displacement is difficult to correct if detected >1 week. Re-xray 4-5 days post-injury.
- Displaced, angulated
- RICE, radial gutter splint as above
- Refer early for pinning
Fractures through the metacarpal head, involving the articular surface, require operative fixation.
References
- Life in the Fast Lane. Boxer’s fracture.
CLINICAL CASES
Bone and Joint Bamboozler
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC