
![]()
Median Nerve Lesions
Median nerve lesions cause weakness in forearm pronation, wrist/finger flexion, and thumb opposition, with characteristic sensory loss in the lateral hand
Median nerve lesions are characterized predominantly by:
- Weak pronation of the forearm
- Weak flexion and radial deviation of wrist
- Inability to oppose the thumb
- Inability to flex the thumb
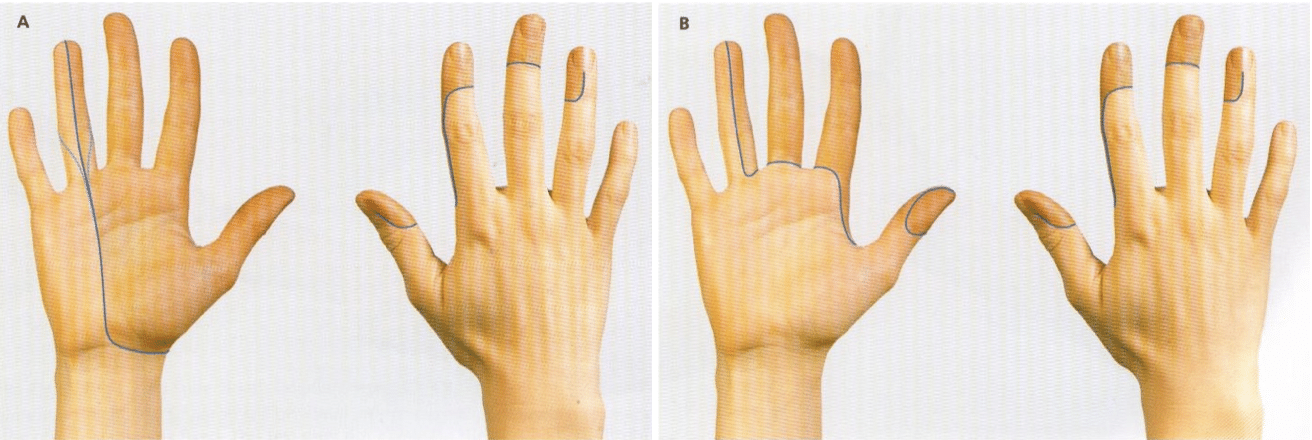
Variable anaesthesia is experienced over:
- Lateral palm
- Lateral 3½ fingers on palmar surface, and distal ½ of the lateral 3½ fingers on the dorsal surface
Lesions at the carpal tunnel will spare palmar sensation.
The most common causes include:
- Trauma (especially at the wrist)
- Compartment syndromes at the carpal tunnel
Investigation and management depend on:
- The cause and location of the lesion
- Acuteness of onset
- Severity of symptoms
Anatomy
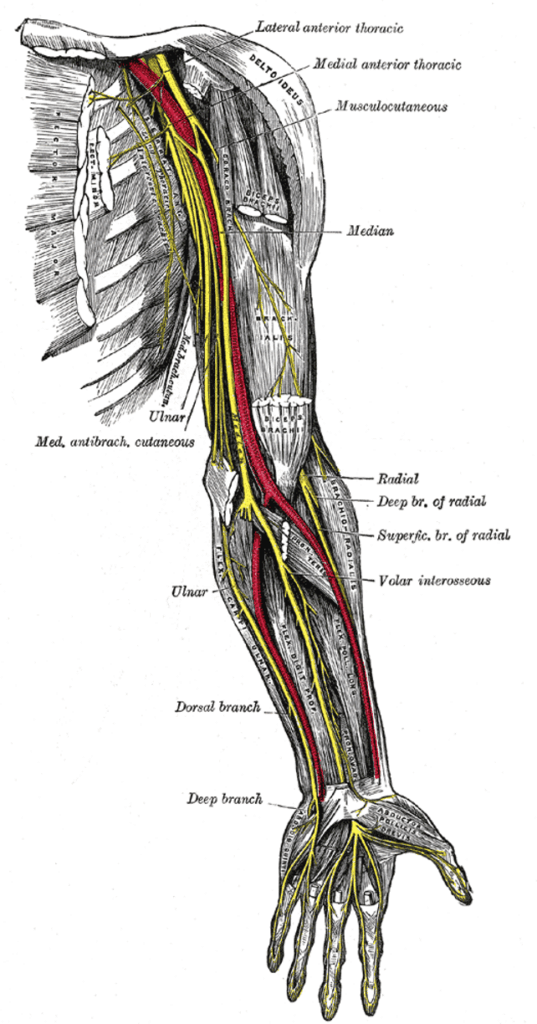
Course of the Median Nerve
- Roots: C5–T1
- Arises from lateral and medial cords of the brachial plexus
- Descends lateral then medial to the brachial artery
- Passes through cubital fossa under bicipital aponeurosis
- Passes between heads of pronator teres and gives off anterior interosseous nerve
- Travels between FDS and FDP
- Emerges at wrist lateral to FDS tendons and behind palmaris longus
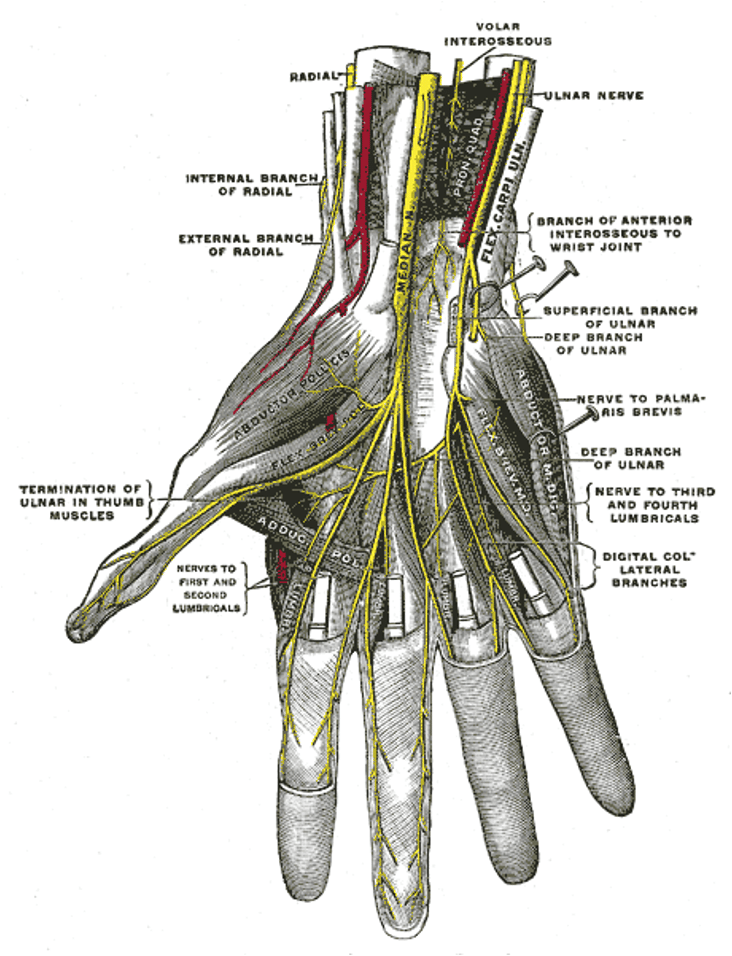
- Enters palm behind flexor retinaculum and divides into lateral and medial branches
- Palmar cutaneous branch arises proximal to flexor retinaculum and remains superficial
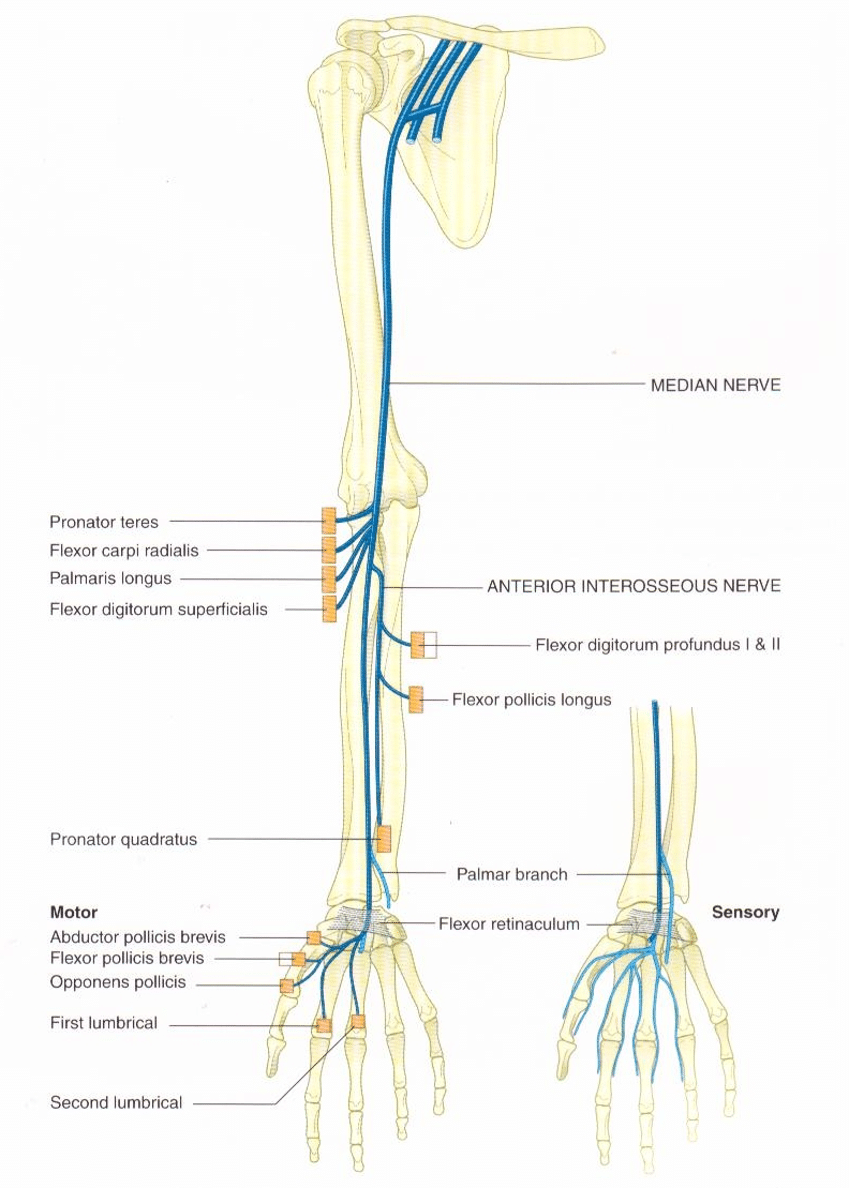
Innervations
Forearm:
- Pronator teres
- Flexor carpi radialis
- Palmaris longus
- Flexor digitorum superficialis
Anterior interosseous nerve:
- Lateral half of FDP (digits I & II)
- Flexor pollicis longus
- Pronator quadratus
Hand:
- Thenar muscles (abductor pollicis brevis, flexor pollicis brevis, opponens pollicis)
- 1st and 2nd lumbricals
- Cutaneous innervation to lateral palm and 3½ lateral fingers (palmar and distal dorsal)
Muscle Actions
| Muscle | Action |
|---|---|
| Pronator teres | Pronates & flexes forearm |
| Flexor carpi radialis | Flexes & abducts wrist |
| Palmaris longus | Flexes hand |
| FDS | Flexes middle phalanx, assists proximal phalanx & wrist flexion |
| FDP (lateral) | Flexes distal phalanx I & II, assists proximal joints |
| Flexor pollicis longus | Flexes distal phalanx of thumb |
| Pronator quadratus | Pronates forearm |
| Thenar muscles | Thumb opposition, abduction, flexion |
| 1st & 2nd lumbricals | MCP flexion & IP extension of index & middle fingers |
Clinical Assessment
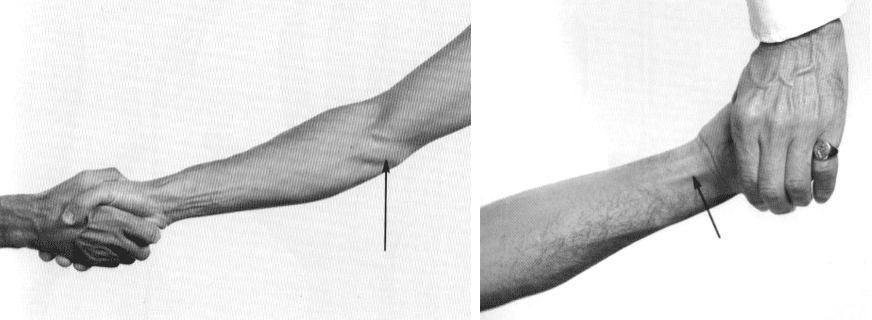
Right: Flexor digitorum profundus I and II, (anterior interosseous nerve C7,8). The patient is flexing the distal phalanx of the index finger against resistance with the middle phalanx fixed.
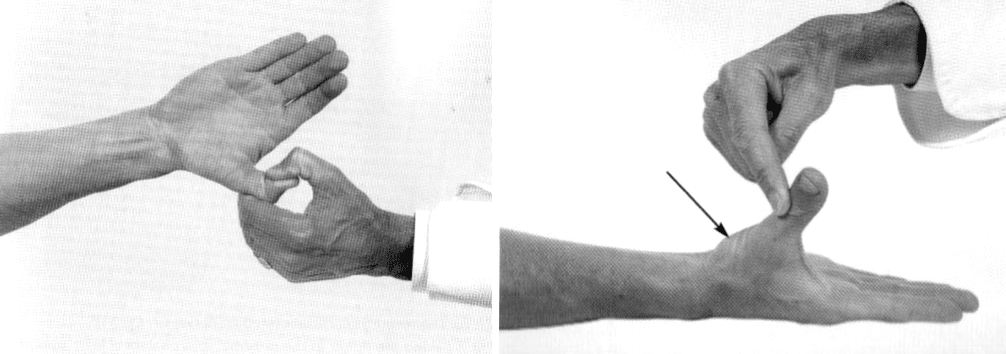
Right: Abductor pollicis brevis, (median nerve C8 T1). The patient is abducting the thumb at right angles to the palm against resistance. Arrow shows the muscle belly which can be felt and seen.
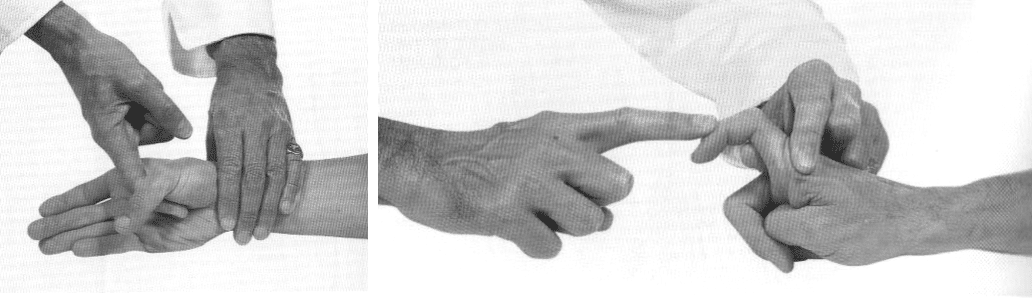
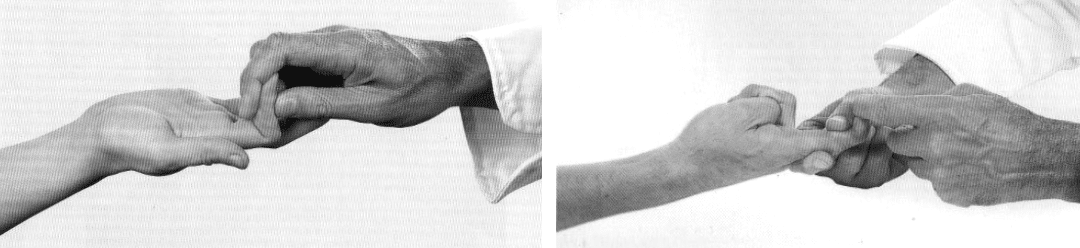
Right: 1st Lumbrical-Interosseous muscle, (median and ulna nerves, C8, T1). The patient is extending the finger at the proximal interphalangeal joint against resistance with the metacarpo-phalangeal joint hyperextended and fixed.
Pathology
Causes
- Trauma:
- Penetrating/blunt injuries
- Fractures/dislocations at wrist (e.g. lunate dislocation)
- Neuropraxia:
- Direct trauma
- Anterior compartment syndrome
- Carpal tunnel syndrome
- Mass lesions:
- Tumours, abscesses
- Neuropathies:
- Mononeuritis (e.g. DM, vasculitis, infections, malignancy)
Median Nerve Deficits
At the Elbow:
- Motor: Loss of forearm pronators and wrist/finger flexors (except FCU, medial FDP)
- Sensory: Loss over lateral palm and 3½ fingers (palmar + distal dorsal)
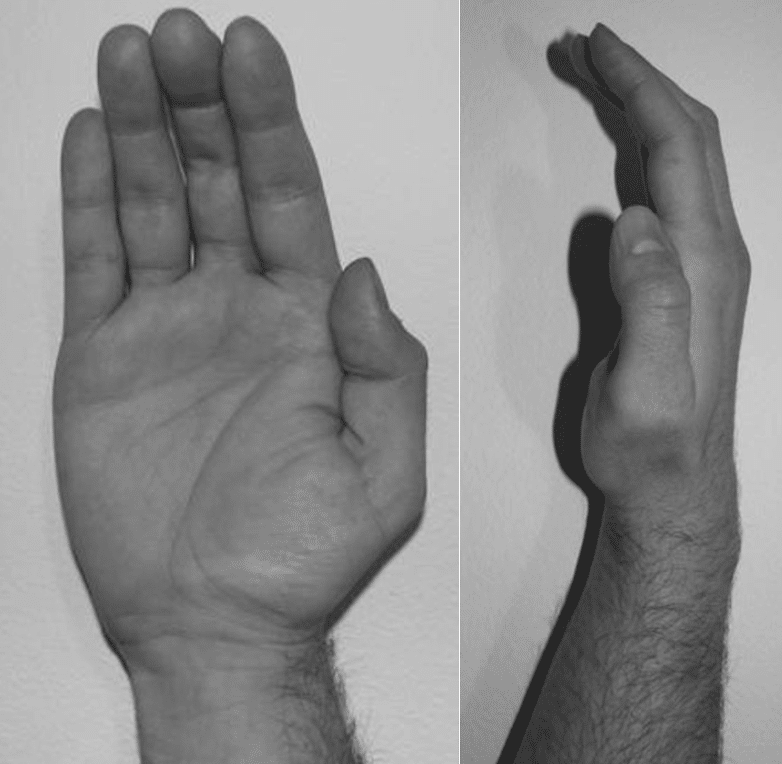
At the Wrist:
- Motor: Thenar muscle paralysis, simian hand deformity, 1st/2nd lumbrical weakness
- Sensory: Same as above
- Main disability: Loss of thumb opposition and lateral finger sensation
Investigations
- Nerve conduction studies:
- Confirm diagnosis, assess extent
- Bloods (as indicated):
- FBC, U&Es, glucose, CRP, ESR, heavy metals
- Imaging:
- CT/MRI for mass lesions or visualisation of nerve/spine (C5–6)
- Biopsy:
- Rare; e.g. for suspected mononeuritis, leprosy
Management
- Treat underlying cause
- Fasciotomy if compartment syndrome
- Occupational therapy: Splints, aids
- Physiotherapy: Rehab or prevent complications
Disposition
Dependent on:
- Cause of the lesion
- Severity of symptoms
- Acuteness of onset
Appendix 1
Median Nerve Anatomy
Appendix 2
Appendix 3
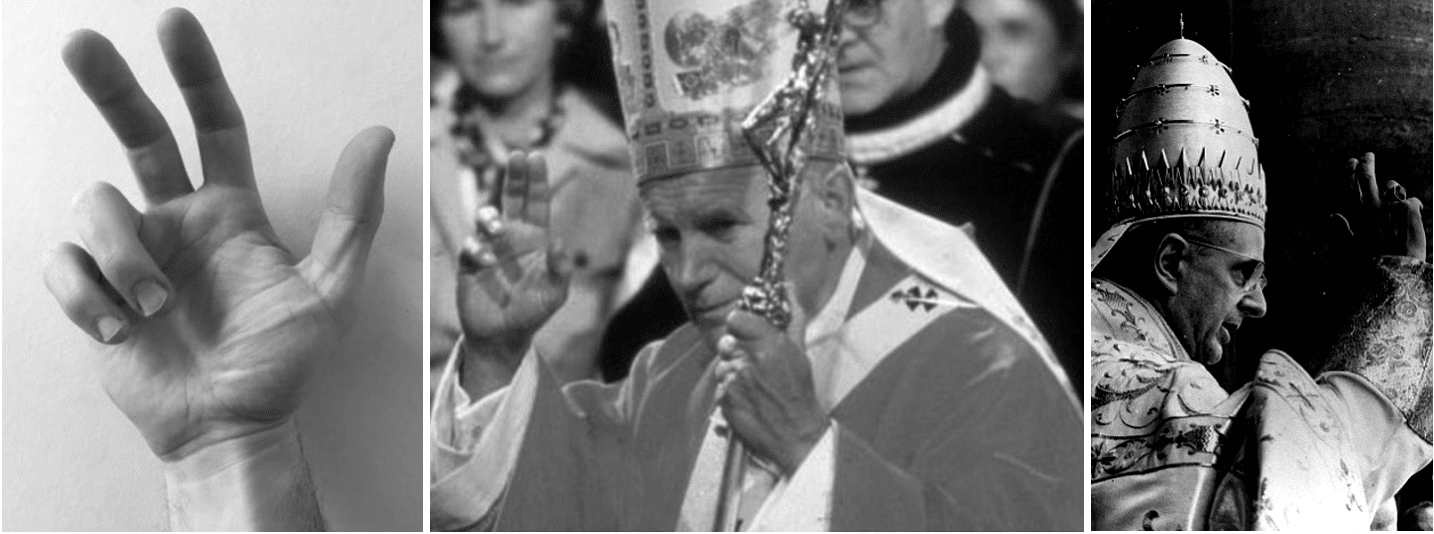
Middle: Pope John Paul II demonstrates a benediction sign, (1982; in Westminster Cathedral).
Right: Pope Paul VI, c. 1975.
References
Publications
- Brazis PW, Masdeu JC, Biller J. Localization in Clinical Neurology. 8e 2021
- Fuller G. Neurological Examination Made Easy. 6e 2019
- O’Brien M. Aids to the Examination of the Peripheral Nervous System. 6e 2023
FOAMed
- Coni R. Neuro 101: Peripheral Nervous System. LITFL
- Nickson C. Myotomes and Differentiating Nerve Lesions. LITFL
Fellowship Notes

MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner

Educator, magister, munus exemplar, dicata in agro subitis medicina et discrimine cura | FFS |