![]()
Nail Gun Injuries
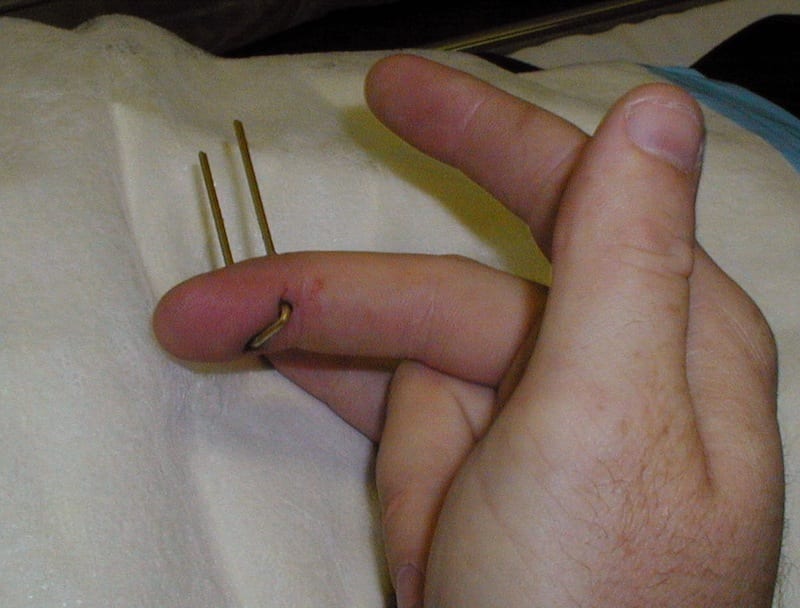
Mr Ivor Plank attended the Emergency Department on the weekend having developed a painfully strong bond with an expensive piece of skirting board…

Nail Gun Injuries:
Nail gun-related injuries are a serious occupational risk with potentially lethal outcomes. Nail guns were introduced in both industry and the general public back in 1959. Nail guns have also been describe as cartridge compression guns, or powered-actuated tools, and are used to fire nails into wood, steel, and masonry.
- 75% of nail gun injuries involve the soft tissues the other 25% involves structural damage
- Fractures, longitudinal tendon split or puncture, joint capsule penetration and neuropraxia
- 65% of nail gun injuries occur in the hand (the majority of injuries caused by nail guns occur on the non-dominant side of the body)
- Other common sites include the head, neck, chest, abdomen, vertebral column, spinal cord, and extremities, have been documented in the literature, with case reports of fatalities being report sporadically.
- Nail gun injuries commonly occur related to improper use by the operator, and not following occupational health and safety requirements for operating a nail gun.
- An Australian study in Victoria looked at emergency department presentations for nail gun injuries showed in a 5 year period (1997-2002)
- 604 case presentations
- 98.5% were male
- 67% involved injuries to the hand
- Admission rate was 23%.
- Bump -firing occurs when the operator holds down the trigger on the nail gun, the gun is then fired by bumping the safety bracket along the workpiece, workers use this methods to speed up delivery, however by following this practice has lead to an increase in the number of nail gun injuries.

Mechanism of injury caused by Nail Guns:
- The nail gun can produce velocities as high as 1,400 feet per second, at which speed a nail can penetrate stressed concrete up to 10cm.
- The amount of energy required to cause serious injury is fairly low: penetration of the skin occurs with projectile velocities of 150 feet per second, whereas bony fractures may occur with projectile velocities of 195 feet per second.
- Mechanisms of nail gun injury include direct penetration , shrapnel wounds from exploding cartridges, and high-pressure injection injuries from the compressed air used to activate the gun.
When nail projectiles penetrate human tissues, the kinetic energy transfers from the object to surrounding tissues, resulting in shock waves that form temporary and permanent cavity spaces. As these shock waves expand, the temporary cavity created causes crush and stretch damage to the tissues. If the projectile shatters bones, these fragments act as secondary missiles, further increasing tissue trauma.
Pierpont, Y. et.al. (2008)
Assessment of Nail Gun Injuries:
- A careful history needs to be taken with special attention paid to the type of nail used (Barbed Vs Non-barbed), mechanism of injury, and time since injury.
Physical assessment should note:
- General appearance of the hand
- Obvious fractures or deformity
- Limitations on range of motion
- Proximity to important structures
- Neurovascular status and capillary refill
Immediate surgical referral should occur if there is evidence of:
- Absent pulses
- An insensate digit
- Suspected joint penetration
- Fractures
- Tendon injuries
Imaging:
- X-rays are the imaging modality of choice, with majority of the literature stating that a lateral and AP X-ray will be able to demonstrate associated fractures, joint penetration, and the presence of metallic barbs on the nail shafts.
- There is no good literature or studies to demonstrate if its better to image before or after removal of the nail, some authors have stated its better to image before if the nail has barbs attached as this will help guide your removal, where other authors have said should X-rays after removal so the true extent of damage can be seen.

Emergency Department Management:
Analgesia:
- Penetrating injuries cause considerable pain and discomfort to the patient, effective analgesia needs to be provided to allow removal of object, investigations and cleaning of the wound.
- For finger injuries, a digital nerve block has been shown to be more effective than a metacarpal block.
- Digital nerve blocks seen to be the most effective means of managing these injuries, and provides better pain relief for the patient.
- The benefit off a digital nerve block over local infiltration of anaesthetic is its perform away from the wound, decreasing risk off further wound contamination.
- Ropivacaine has been shown to provide longer analgesia/anaesthetic when compared to lidocaine.
- Other options available in the emergency department to provide analgesia include: procedural sedation, Nitrous Oxide, Oral and Parenteral opiods.
Irrigation and washout:
- The wound needs a thorough wash out either in emergency department or if complex during theatre.
- Personally I recommend irrigating with normal saline first to clean away any debris and prevent infection, using saline over povidone-iodine based solutions initially allows for good visualisation of the wound, as povidone-iodine will causes staining of the wound.
- There are no studies looking at povidone-iodonine based solutions in prevention of infection in acute wounds, however in elective surgery cases it has been shown to be off benefit.
- I would recommend once a definitive plan for the wound has been made that the wound is cleaned and irrigated with an antibacterial solution like povidone-iodine, as the benefit will most probably out-weigh any of the harm it may cause. Its effective against gram positive and negative bacteria, spores, fungi, viruses and protozoa.
- Povidone-iodine solutions should only be used in the initial management of acute wounds as they prevent new tissue from granulating.
- The pressure needed to adequately irrigate a wound should be 5 to 8 psi and may be achieved with a 16-19gauge needle attached to a 35-65ml syringe.
- Although normal saline is the preferred irrigation fluid, tap water has shown be just as effective, with no significant increase in infection, and is a cheaper option.
Tetanus Prophylaxis:
- Adults who have sustained injuries deemed to be tetanus prone should receive a ADT booster, if more than 5 years have elapsed since their last dose.
What constitutes a tetanus prone wound:
- Compound fractures
- Bite wounds
- Deep penetrating wounds
- Wounds containing foreign bodies
- Wounds complicated by pyrogenic infections
- Burns
- Superficial wounds contaminated with soil, dust, or horse manure
- Avulsed tooth
Antibiotics:
- The use of antibiotics in wound healing is a very contentious issue in emergency medicine, with some studies showing in simple wounds they provide no benefit, however the jury is still out when it comes to complex, contaminated wounds, with limited good studies to support their use, and lots of anecdotal cases that recommend giving antibiotics.
- Meticulous wound management early cleaning, irrigation and debridement has shown to be more effective at decreasing infection rates than antibiotics alone.
- A study of 88 patients with nail gun injuries showed 84% received intravenous antibiotics in hospital, 75% of these patients were discharged home with a course of oral antibiotics. 3 of the 88 patients went on to develop infection.
- It’s generally recommended patients receiving operative repair and nail removal in theatre should receive pre and post operative antibiotics.
Referral and follow up:
- The majority of nail gun injuries to the extremities, where there is no intra-articular involvement, and no presence or risk of neurovascular compromise, can be managed with simple extraction and minimal debridement, and discharge with a short course of cephalosporin antibiotics depending on local institutional practise.
- Referral to plastics or hand surgeons if suspicion of injury to the joint space, tendons, or neurovascular bundles, so intra-operative exploration can occur.
- Patients discharged from the emergency department should have follow up arranged within 48-72 hours either by their primary care physician or plastics/orthopaedic clinic to monitor for return of function and wound healing.
Medico-Legal Pitfalls
- Its difficult to define a standard of care in wound management as there is limited evidence based studies, and most of what we do in the emergency department is anecdotal.
Common Pitfalls include:
- Failing to X-ray wounds for retained foreign bodies
- Failing to provide/recommended early follow up to assess wound healing
- Wounds at high risk of infection, not allowing delayed closure of the wound
- Failing to provide and document a neuro-vascular assessment, always document intact motor and sensory sensation
Reference:






- Bitzos, I. Granick, M. (2009). Management of Penetrating Wrist Injuries in the Emergency Department. Eplasty. 468-473.PMID: 19956570
- DeBoard, R. et.al. (2007). Principles of Basic Wound Evaluation and Management in the Emergency Department. Emergency Medicine Clinics of North America. 25, 23-29.PMID: 17400071
- Hart, R. Uehara, D. & Wagner, M. (2001). Emergency and Primary Care of the Hand. Dallas Texas: American College of Emergency Physicians.
- Hoffman, D. & Adams. (2003). Antimicrobial management of mutilating hand injuries. Hand Clinics. 33-39. PMID: 12683444
- Hoffman, D. Jebson, P. Steyers, C. (1997). Nail Gun Injuries of the Hand. American Family Physician. 56(6), 1643-1647. PMID: 9351432
- Horne, B. & Corley, F. (2007). Review of 88 nail gun injuries to the extremities. Injury. 39, 357-361.PMID: 17996238
- Knott, J. McR Meyer, A. & Kas, P. (2004). Nail gun-related injuries presenting to the emergency department. Emergency Medicine Australasia. 16, 254-255.PMID: 15228478
- Mckirdy, S. & Carley, S. (2001). Digital or metacarpal block for finger injuries. bestbets.org
- Nakamura, Y. & Daya, M. (2007). Use of Appropriate Antimicrobials in Wound Management.Emergency Medicine Clinics of North America. 25, 156-176.PMID: 17400079
- Osborne, C. & Kelsey, M. (2008). Do povidone-iodine (betadine) soaked dressing reduces the rate of infections in open wounds? www.bestbets.org
- Patel, P. & Miller, M. (2007). Postcare Recommendations for Emergency Department Wounds.Emergency Medicine Clinics of North America. 25, 147-158.PMID: 17400078
- Pfaff, J. & Moore, G. (2007). Reducing Risk in Emergency Department Wound Management.Emergency Medicine Clinics of North America. 25, 189-201.PMID: 17400081
- Pierpont, Y. Pappas-Politis, E. Naidu, D. Salas, E. Johnson, E. & Payne, W. (2008). Nail-Gun Injuries to the Hand. Eplasty. 479-488.PMID: 19079574
- Singisetti, K. Kokkinakis, M. & Shankar, N. (2008). Penetrating injury of the hand with a door handle: a case report. Journal of Medical Case Reports. 377(2), 1-3.PMID: 19063727
- The Australian Immunisation Handbook 9th ed. (2008). Australian Government; Department of Health and Ageing:Canberra.
- Thomas, M. & Jones, S. (2001). Antibiotics and compound finger fractures. bestbets.org
[cite]
Trauma Library
Injury database
Emergency nurse with ultra-keen interest in the realms of toxicology, sepsis, eLearning and the management of critical care in the Emergency Department | LinkedIn |
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |