
![]()
Neuro 101: Cranial Nerves
A brief overview of the cranial nerves, their function, methods of testing and common pathology
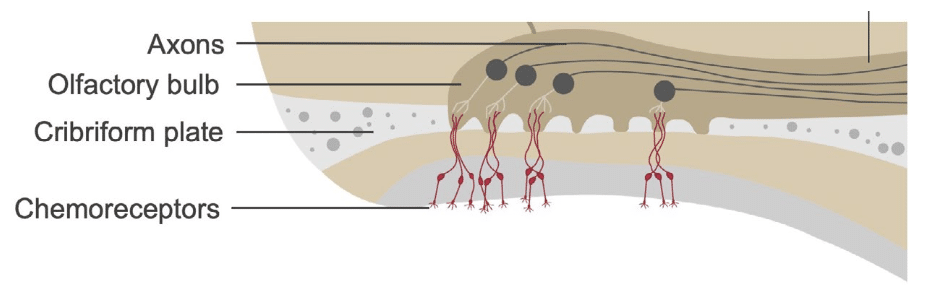
Olfactory Nerve (CN I)
Function: Responsible for the sense of smell.
Testing: Use common, non-irritating scents (e.g. mint, spices, flavoured toothpaste). Avoid volatile or noxious chemicals.
Common Pathology: Loss of smell (anosmia) may result from head trauma, subfrontal or olfactory groove meningiomas, or neurodegenerative diseases such as Parkinson’s disease.
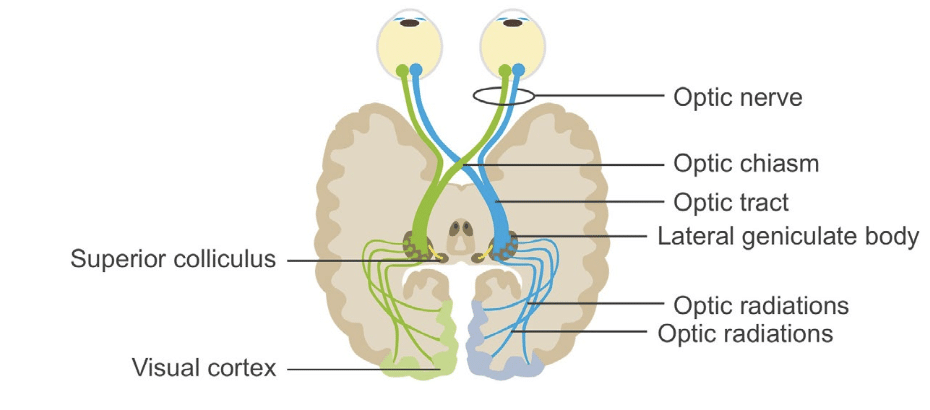
Optic Nerve (CN II)
Function: Vision; afferent pathway for the pupillary light reflex.
Testing: Assess visual acuity, visual fields, and pupillary light reflex (direct and consensual). Perform fundoscopy.
Note: Regarding the pupillary light reflex:
- Afferent Pathway: Begins with light stimulation of the retina, travels through the optic nerve to the pretectal area of the midbrain.
- Efferent Pathway: Starts from the Edinger-Westphal nuclei, uses the oculomotor nerve to reach the ciliary ganglion, and finally innervates the iris sphincter muscles
Common Pathology:
- Optic neuritis (causes blurred vision, eye pain, afferent pupillary defect);
- Chiasmal lesions (e.g. pituitary tumours causing bitemporal hemianopia).
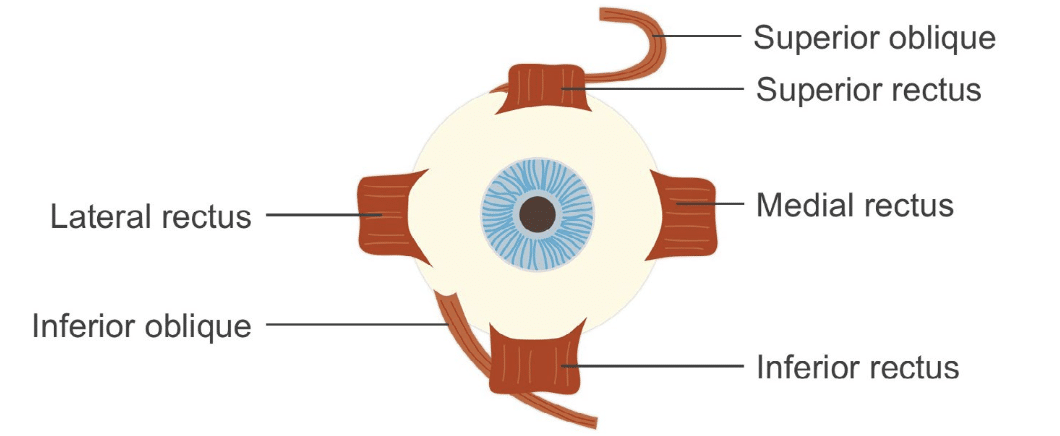
Oculomotor, Trochlear, and Abducens Nerves (CN III, IV, VI)
Function: Control extraocular eye movements.
- CN III innervates the superior, medial, and inferior recti, inferior oblique, and levator palpebrae;
- CN IV innervates superior oblique;
- CN VI innervates lateral rectus
- CN III also mediates the efferent limb of the pupillary light reflex;
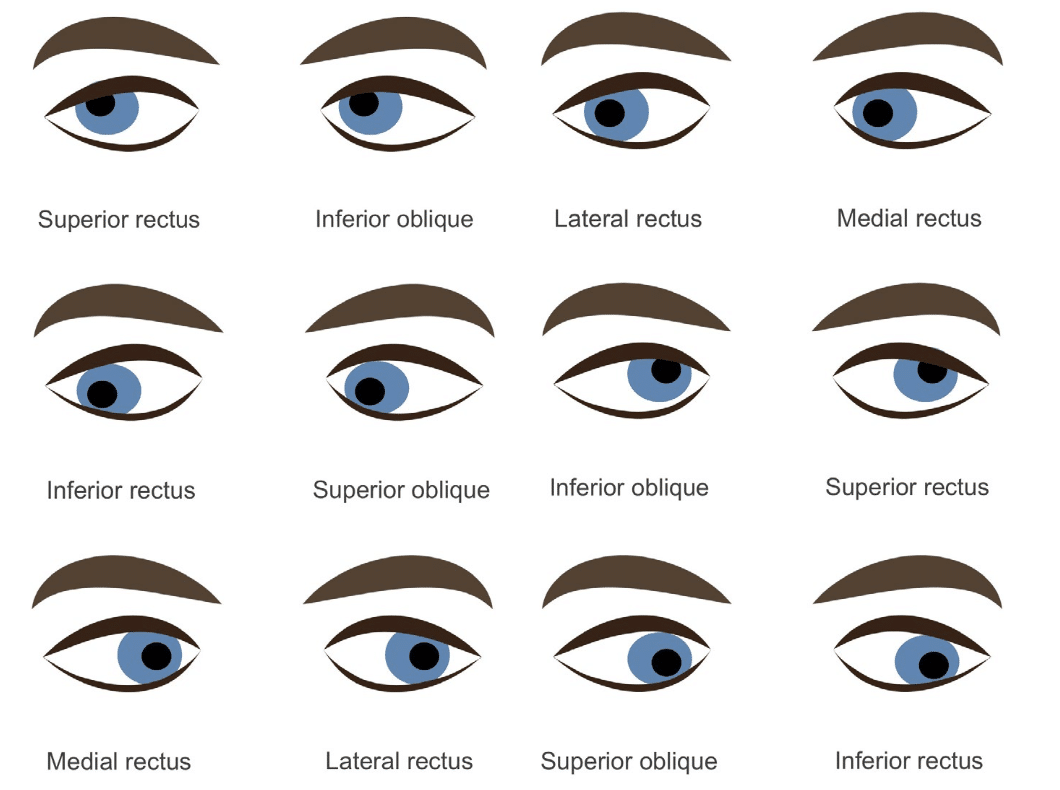
Testing: Assess eye movements through the cardinal planes of gaze, looking for conjugate movement, nystagmus, and accommodation response. Perform red glass test and pupillary light reflex.
Common Pathology:
- CN III: Diabetic oculomotor palsy (pupil-sparing), posterior communicating artery aneurysm (pupil-involving), uncal herniation (fixed dilated pupil and coma), stroke, myopathies.
- CN IV: Head trauma, aneurysm, tumour. Presents with vertical diplopia and inability to look down/in.
- CN VI: Causes include trauma, cavernous sinus thrombosis, cerebellopontine angle tumours. Causes horizontal diplopia and impaired abduction.
Common eye movement abnormalities:
Dysconjugate gaze
- Eyes don’t move synchronously
- Produces double vision
Vertical gaze
- Superior and inferior rectus muscles
- Controlled by oculomotor nerve (CN III)
- Coordinated movement involves superior colliculus
- Altered in Parinaud syndrome (pressure on superior colliculus)
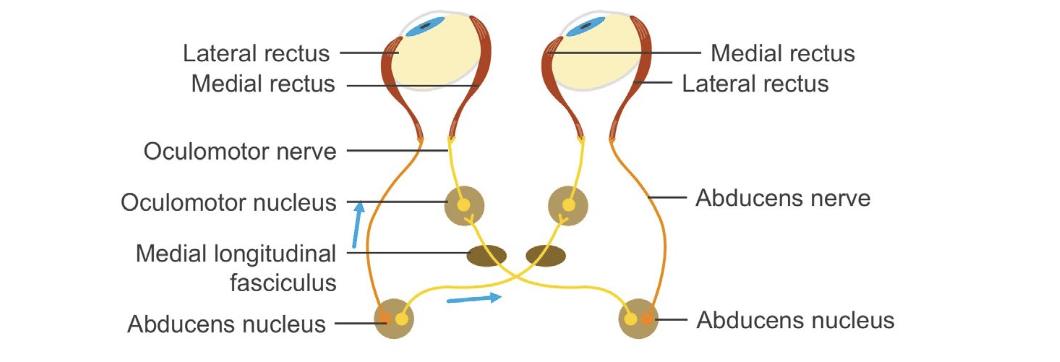
Horizontal gaze
- Involves coordination between CN III and CN VI (innervating medial and lateral rectus muscles respectively)
- Involves coordination through the medial longitudinal fasciculus (MLF)
- Affected in internuclear ophthalmoplegia
- Isolated lesion of medial longitudinal fasciculus (MLF)
- normal abduction but inability to adduct
- nystagmus in adducting eye
- convergence is normal
Vestibular influences on gaze
- CN VIII sends data from vestibular nuclei into MLF; helps keep eyes stable with head turning
- Cortical stroke – patient looks toward lesion
- Brainstem stroke – patient looks away from lesion
- Testing vestibular reflex – oculocephalic maneuver; ice water cold caloric testing
Trigeminal Nerve (CN V)
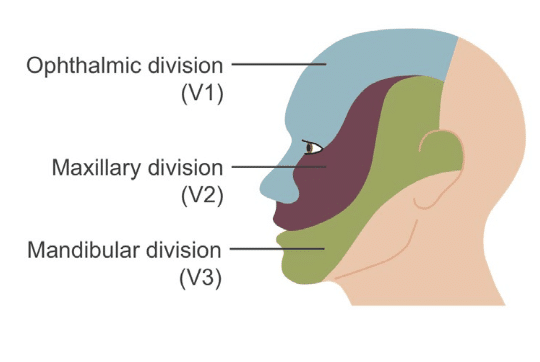
Function: Sensation of face (light touch, pain, temperature, vibration); motor to muscles of mastication and tensor tympani; afferent limb of corneal reflex.
Testing: Assess sensory modalities in V1, V2, and V3 distributions; test corneal reflex and jaw jerk; inspect for muscle wasting.
Common Pathology: Trigeminal neuralgia, cerebellopontine angle tumours, cavernous sinus thrombosis, zoster ophthalmicus.
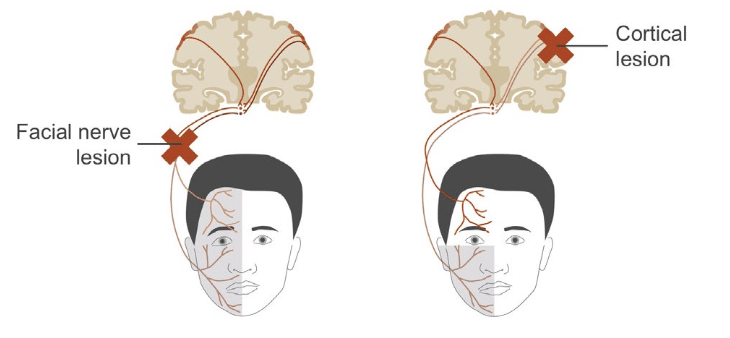
Facial Nerve (CN VII)
Function: Muscles of facial expression, stapedius muscle, taste (anterior two-thirds of tongue), lacrimation, salivation, and sensation over the external auditory canal.
Testing: Observe facial symmetry at rest and during voluntary movements (smiling, eye closure, whistling); look for Bell’s phenomenon.
Common Pathology: Bell’s palsy (LMN lesion with upper and lower facial weakness), Ramsay Hunt syndrome, pontine strokes.
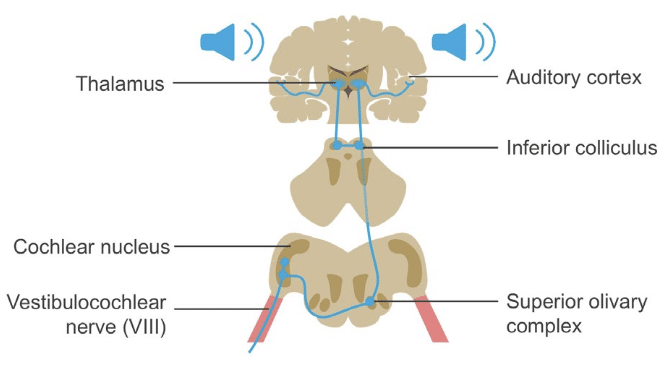
Vestibulocochlear Nerve (CN VIII)
Function: Hearing and balance.
Testing:
- Auditory tests (whisper, finger rub, tuning fork tests such as Weber and Rinne);
- Vestibular tests (Dix-Hallpike, head impulse test, gait observation)
Common Pathology:
- Vestibular neuritis,
- Acoustic neuroma (cerebellopontine angle tumours)
- Vertigo
- Deafness (sensorineural or conductive)
- Peripheral (labyrinthine)
Glossopharyngeal and Vagus Nerves (CN IX and X)
Function:
- CN IX: Taste/sensation to posterior third of tongue, pharyngeal sensation, swallowing, salivation, carotid body and sinus input, afferent gag reflex.
- CN X: Palatal elevation, speech, swallowing, autonomic innervation of thoracic/abdominal viscera, somatic sensation of external auditory canal, efferent gag reflex.
Testing:
- Gag reflex; palatal elevation, uvula position (deviation away from side of lesion)
- Cough strength
- Voice quality (hoarseness)
- Carotid sinus reflex
Common Pathology: Glossopharyngeal neuralgia, jugular foramen syndromes, cerebellopontine angle tumours.
Spinal Accessory Nerve (CN XI)
Function: Motor to sternocleidomastoid and trapezius; via recurrent laryngeal nerve contributes to laryngeal motor function.
Testing: Shoulder shrug and head rotation against resistance (weakness of sternocleidomastoid and / or trapezius)
Common Pathology: Injury during neck surgery, jugular foramen compression (e.g. tumours), recurrent laryngeal nerve injury causing hoarseness.
Hypoglossal Nerve (CN XII)
Function: Tongue movement.
Testing: Observe tongue at rest for atrophy or fasciculations; ask patient to protrude tongue (deviation towards side of weakness); assess strength by pushing tongue against cheek.
Common Pathology: Stroke, tumours, motor neuron disease, Huntington’s disease, meningeal or cerebellar disorders, essential tremor.
| Cranial Nerve | Function | Testing | Common Pathology |
|---|---|---|---|
| Olfactory (CN I) | Smell | Use common scents (avoid volatile chemicals) | Head trauma, meningioma, Parkinson’s disease |
| Optic (CN II) | Vision; Afferent pupillary light reflex | Visual acuity, pupillary reflex, fundoscopic exam | Optic neuritis, chiasmal lesions (bitemporal hemianopsia) |
| Oculomotor (CN III) | Extraocular movement; pupil constriction; eyelid elevation | Cardinal gaze, pupillary light reflex | Diabetic palsy, PCA aneurysm, uncal herniation |
| Trochlear (CN IV) | Superior oblique muscle (eye down/in) | Cardinal gaze | Head trauma, aneurysm, vertical diplopia |
| Abducens (CN VI) | Lateral rectus muscle (eye abduction) | Cardinal gaze | Orbital trauma, cavernous sinus thrombosis |
| Trigeminal (CN V) | Facial sensation; muscles of mastication | Sensory exam, corneal reflex, jaw jerk | Tumours, sinus thrombosis, trigeminal neuralgia |
| Facial (CN VII) | Facial muscles, taste anterior 2/3 tongue, lacrimation | Symmetry, expressions, Bell’s phenomenon | Bell’s palsy, Ramsay Hunt syndrome |
| Vestibulocochlear (CN VIII) | Hearing; balance | Rinne/Weber, Dix-Hallpike, head impulse | Tumours, deafness, vertigo |
| Glossopharyngeal (CN IX) | Taste posterior 1/3, swallowing, gag reflex | Gag reflex, speech, carotid reflex | Neuralgia, CPA tumours, jugular foramen lesions |
| Vagus (CN X) | Speech, swallowing, parasympathetic control | Gag reflex, palatal elevation, cough | Same as CN IX |
| Accessory (CN XI) | SCM and trapezius movement | Shoulder shrug, head turn | Jugular foramen compression, neck surgery |
| Hypoglossal (CN XII) | Tongue movement | Protrusion, strength, fasciculations | Stroke, MND, cerebellar disease, essential tremor |
Clinical Neurology Essentials
- Coni R. Neuro 101: Neurological Examination. LITFL
- Coni R. Neuro 101: Cerebral Hemispheres. LITFL
- Coni R. Neuro 101: Cerebellum and Basal Ganglia. LITFL
- Coni R. Neuro 101: Brainstem. LITFL
- Coni R. Neuro 101: Cranial Nerves. LITFL
- Coni R. Neuro 101: Spinal Cord. LITFL
- Coni R. Neuro 101: Peripheral Nervous System. LITFL
References
Further reading
- Brazis PW, Masdeu JC, Biller J. Localization in Clinical Neurology. 8e 2021
- Campbell WW. DeJong’s The Neurologic Examination. 8e 2019
- Fuller G. Neurological Examination Made Easy. 6e 2019
- Kiernan J. Barr’s The Human Nervous System: An Anatomical Viewpoint. 10e 2015
- O’Brien M. Aids to the Examination of the Peripheral Nervous System. 6e 2023
- Patten JP. Neurological Differential Diagnosis. 2e 1996
- Waxman SG. Correlative Neuroanatomy. 23e 1996
Publications
- Biousse V, Newman NJ. Ischemic Optic Neuropathies. N Engl J Med. 2015 Jun 18;372(25):2428-36.
- Kattah JC, Talkad AV, Wang DZ, Hsieh YH, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke. 2009 Nov;40(11):3504-10.
- Kwong Yew K, Abdul Halim S, Liza-Sharmini AT, Tharakan J. Recurrent bilateral occipital infarct with cortical blindness and anton syndrome. Case Rep Ophthalmol Med. 2014;2014:795837.
Neurology Library

Robert Coni, DO, EdS, FAAN. Vascular neurologist and neurohospitalist and Neurology Subspecialty Coordinator at the Grand Strand Medical Center in South Carolina. Former neuroscience curriculum coordinator at St. Luke’s / Temple Medical School and fellow of the American Academy of Neurology. In my spare time, I like to play guitar and go fly fishing. | Medmastery | Linkedin |