
![]()
NOACs
The NOACs, new oral anticoagulants (although not so new now) have been promoted as equivocal or if not better than warfarin for anticoagulation. Certainly from a consumer point of view it is far easier to manage than clean loading and INR checks. From the critical care world it has been confusing, distressing, sometimes hopeless when trying to deal with a life treating bleed while on these medications. There is very limited data on deliberate self poisoning and hence this page will focus more on the management of bleeding and potential reversal products on the market.
Toxic Mechanism + Toxicokinetics:
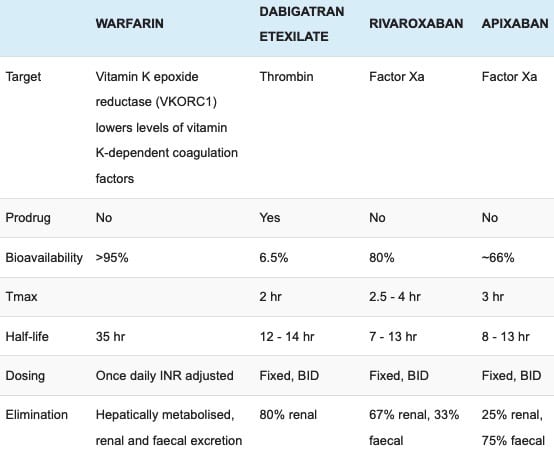
- Dabigatran – has a ‘T’ in the name therefore it is a direct THROMBIN inhibitor
- Apixaban and rivaroxaban – Xa in the name therefore a direct Xa inhibitor
Resuscitation:
- Rarely required
- Uncontrolled or life threatening haemorrhage:
- Apply local control measures
- Institute haemodynamic support and give blood products as indicated
- Due to this evolving field a number of products have been used. Listed below is the latest approach to what is considered most effective. Understandably PCC, FFP and factor VII (increased risk of thromboembolism in the elderly) have all been used in varying cases, you should administer coagulation factors as per local guidelines and haematology advice:
- Dabigatran
- Tranexamic acid 1 gram intravenous followed by 1 gram infusion over 8 hours.
- Activated PCC – factor eight inhibitor bypassing activity (FEIBA – available in the USA).
- Inactivated PCC has a very limited effect.
- Haemodialysis – see below
- Antidote – see below
- Apixaban and Rivaroxaban
- Tranexamic acid 1 gram intravenous followed by 1 gram infusion over 8 hours.
- Inactivated prothrombin complex concentrate
- Activated PCC – factor eight inhibitor bypassing activity (FEIBA – available in the USA)
- Dabigatran
Risk Assessment
- Any quantity of NOACs ingested could result in significant bleeding
- Renal impairment will prolong the elimination half-life in all the NOACs.
- Currently there is no support in giving pro-thrombotic factors in the absence of bleeding.
- Clinical features:
- Usually asymptomatic.
- Severe coagulopathy may present as bruising, petechial or puerperal rashes, gingival bleeding, epistaxis, gastrointestinal bleeding or haematuria.
- If there are no other ingestants then an altered GCS must prompt consideration for an intracranial bleed.
- Children: There are no reports of ingestion of NOACs in children as yet but even 1 or 2 tablets will result in significant anticoagulation.
Supportive Care
- General supportive measures
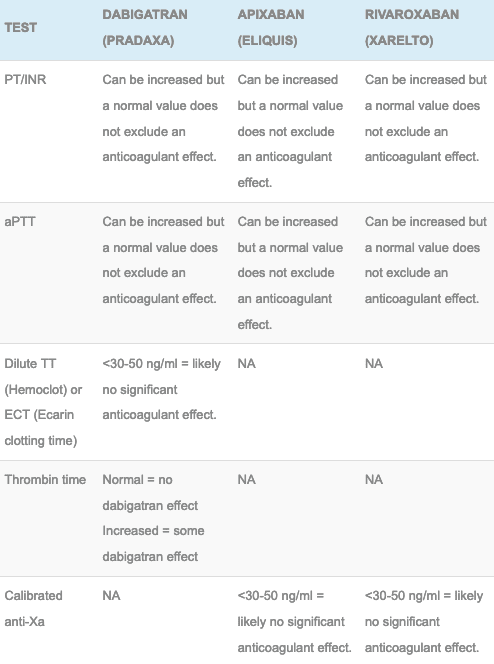
Investigations
- Screening: 12 lead ECG, BSL, Paracetamol level
- Specific:
- FBC, EUC, Serum calcium, Liver function tests, Blood group and antibody screen
- Point of care (POC) testing has not been validated – do not use it
Decontamination:
- Activated charcoal can be used for an acute overdose or a patient who is bleeding who has taken a recent dose:
- Most effective within 2 hours
- Variation in the literature would suggest some benefit of charcoal out to 6 hours but this is limited and largely studied with apixaban (no human data on dabigatran).
Enhanced Elimination
- Dabigatran can be removed by haemodialysis. This should be considered early in an acute overdose or in a patient with hemorrhagic complications on dabigatran. Removes approximately 60% over 2 – 3 hours. The haemodynamic stability of the patient will determine if this is feasible.
- Apixaban and rivaroxaban are highly protein bound and thus are unlikely to be successfully dialysed.
Antidote
- Dabigatran = Idarucizumab (Praxabind)
- Apixaban and rivaroxaban = watch this space (Andexanet Alfa – reverses effect while infusion is running but rebounds on completion, further data expected 2022 – ANNEXA-4 trial)
- An antidote to rule them all??? Aripazine (PER977) is currently being studied that will reverse oral Xa inhibitors, direct thrombin inhibitors, unfractionated heparin and LMWH. I suspect it will be a longtime before this emerges.
Disposition
- All patients who have overdosed need admission for observation and serial anticoagulation studies until normalised.
- All patients who are bleeding are treated and managed in a suitable area.
- Dabigatran overdose should be managed in a facility capable of haemodialysis.
- In the absence of specific levels patients who have overdosed on dabigatran are medically cleared if the INR and aPTT remain normal 12 hours post ingestion.
- In the absence of specific levels patients who have overdosed on apixaban or rivaroxaban are medically cleared if the PT and aPTT remain normal 12 hours post ingestion.
References and Additional Resources:
Additional Resources:
- CCC – Rivaroxiban and bleeding
- CCC – Dabigatran and bleeding
- CCC – New Oral Anticoagulants
References:
- Chiew AL, Khamoudes D, Chan BS. Use of continuous vena-venous hemofiltration therapy in dabigatran overdose. Clinical Toxicology 2014; 52:283-287
- Hu TY, Vaidya VR, Asirvatham SJ. Reversing anticoagulant effects of novel oral anticoagulants: role of ciraparantag, andexanet alfa, and idarucizumab. Vast Health Risk Manag. 2016; 12:35-44
- Koscielny J, Rutkauskaite E. Rivaroxaban and haemostasis in emergency care. Emergency Medicine International 2014; Feb 20
- Kumar R, Smith RE, Henry BL. A review of and recommendations for the management of patients with life-threatening dabigatran-associated haemorrhage: a single-centre university hospital experience. J Intensive Care Medicine 2014; Mar 25
- Wood P. New oral anticoagulants: an emergency department overview. Emergency Medicine Australasia 2013; 25:503-514

Toxicology Library
DRUGS and TOXICANTS
Dr Neil Long BMBS FACEM FRCEM FRCPC. Emergency Physician at Kelowna hospital, British Columbia. Loves the misery of alpine climbing and working in austere environments (namely tertiary trauma centres). Supporter of FOAMed, lifelong education and trying to find that elusive peak performance.