
![]()
Not just a PE
aka Pulmonary Puzzler 002
This 25 year old female presented with worsening breathless. She has no previous medical problems. Her Chest X-ray is shown below.

Questions
Q1.Describe the chest X-ray findings.
Answer and interpretation
This chest X-ray is normal (or so the radiologist says)
The pulse oximeter reads 90% so you decide to perform a blood gas:
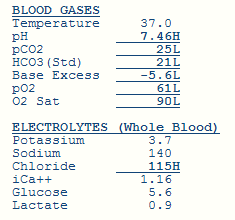
Q2. What does the blood gas show?
Answer and interpretation
- Firstly, the pulse oximeter is accurate!
- Secondly, the patient is sick.
- Thirdly, the patient has a marked respiratory alkalosis (i.e. she is breathing hard).
- Fourthly, the A-a gradient is markedly widened.
After careful consideration of the diagnostic possibilities you decide to perform a CTPA:

Q3. What does the CTPA demonstrate?
Answer and interpretation
Surprise, surprise… a pulmonary embolism (if someone shows you a CTPA and asks you what it shows this is usually the correct answer).
Of particular note, the pulmonary trunk is larger than the aorta. This is often indicates the presence of elevated right ventricular systolic pressure.
Before anticoagulating the patient you review the blood tests:

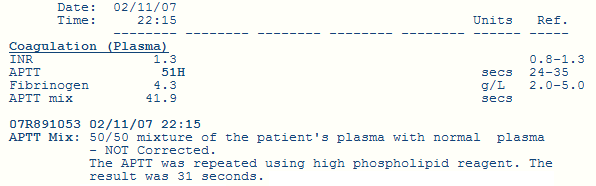
Q4. Describe the significant abnormalities. What is the diagnosis?
Answer and interpretation
- Thrombocytopenia is significant (given the need to anti-coagulate).
- The presence of an elevated APPT that corrects with high phospholipid reagent is seen in antiphospholipid syndrome and thrombocytopenia is also a feature of this condition.
Q5. How would you treat this patient? (by the way the answer is not to ask someone else from another speciality what to do)
Answer and interpretation
The conundrum here is what to do about a life threatening pulmonary embolism is a patient with no platelets. One option is to treat the low platelets so that you can anticoagulate the patient safely.
Thrombocytopenia often gets better with steroids in this condition.
While waiting for the steroids to work you need to make sure that patient doesn’t drop dead from a further pulmonary embolism so you order an ultrasound of the legs to assess the situation further.
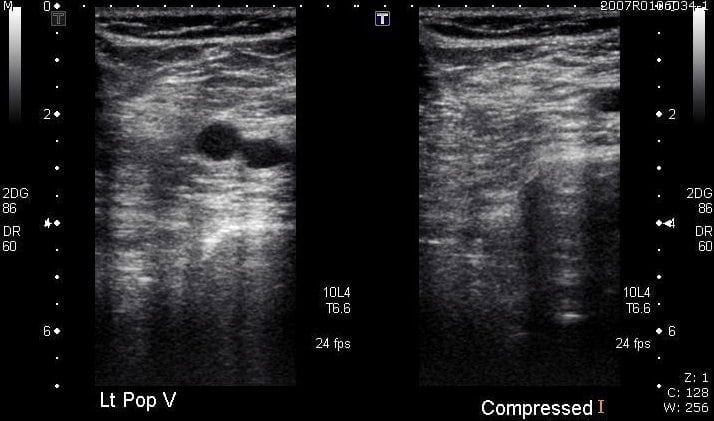
Q5. What does the ultrasound demonstrate?
Answer and interpretation
This ultrasound scan shows a normal vein which disappears with compression.
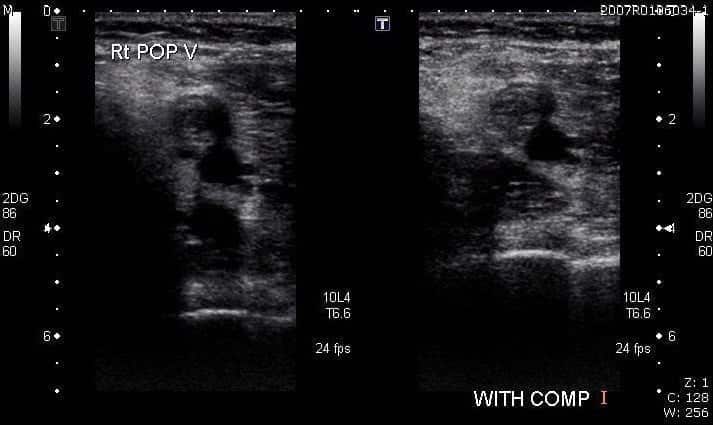
The other leg looks like this because there is a DVT.
Q6. What is this?

Answer and interpretation
An IVC filter to stop the DVT from the leg travelling to the pulmonary artery while waiting for the steroids to kick in.
Q7. Describe the ECG
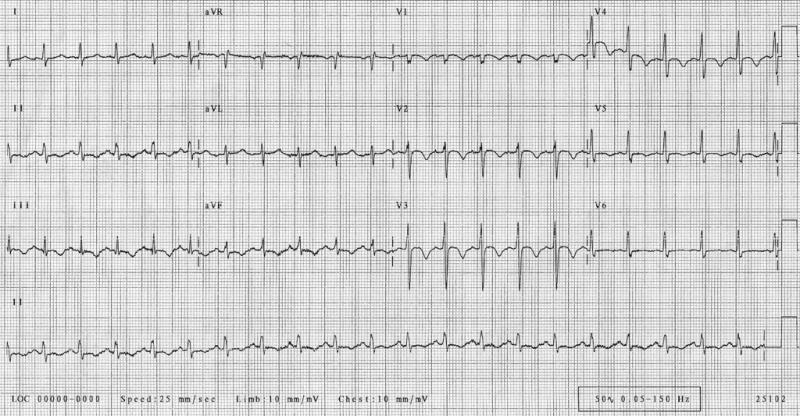
Answer and interpretation
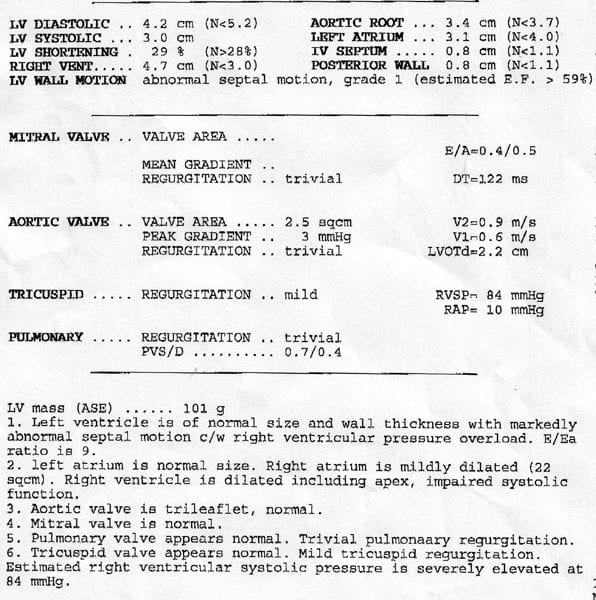
This ECG demonstrates right ventricular strain with T wave inversion in the anterior leads.
The echo report confirms the presence of right ventricular strain:
References
- For more Pulmonary cases check out the LITFL Top 150 Chest X-Rays

CLINICAL CASES
Pulmonary Puzzler
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC