
![]()
Phalen test
Phalen sign is reproduction or exaggeration of numbness and paraesthesia in the median nerve distribution of the hand after sustained wrist flexion. The Phalen test is used as a provocative manoeuvre in suspected carpal tunnel syndrome.
The Phalen test(s)
The original Phalen wrist-flexion test was described by George Smith Phalen (1911–1998) in 1948. Subsequent clinical teaching introduced modified Phalen wrist-flexion variants, most commonly the dorsum-to-dorsum posture. The reverse Phalen test, or Wormser test, is a separate wrist-extension manoeuvre.
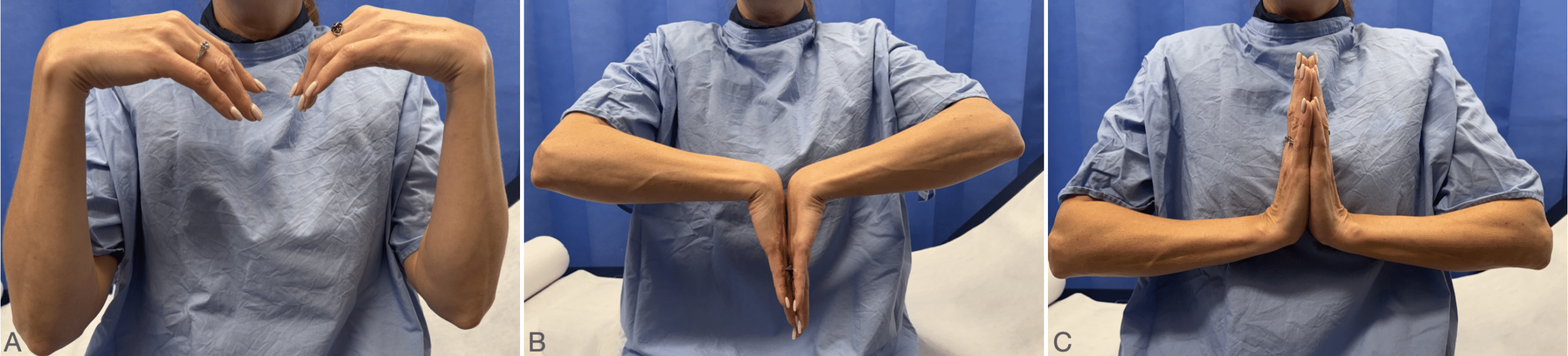
A. Classic Phalen wrist-flexion test: forearms vertical, wrists allowed to fall freely into flexion, hands not touching.
B. Modified Phalen test: dorsal surfaces of the hands placed together to maintain bilateral wrist flexion.
C. Reverse Phalen / Wormser test: palms together with wrists extended.
Classic Phalen test / wrist-flexion test (1948)
Phalen originally described the manoeuvre as the wrist-flexion test. The patient places the flexed elbows on a table, holds the forearms vertically, and allows the hands to fall freely into maximum wrist flexion. The fingers remain extended; the hands do not touch and are not forced into flexion by the patient or examiner. A positive test reproduces or worsens median-distribution symptoms, usually within 30–60 seconds.

Phalen explained the mechanism as increased compression of the median nerve within the carpal tunnel. In wrist flexion, the nerve is compressed between the proximal edge of the transverse carpal ligament and the adjacent flexor tendons and radius. In a normal hand, prolonged wrist flexion may eventually produce tingling; in carpal tunnel syndrome, symptoms are provoked more rapidly.
In performing the so called wrist-flexion test, the patient is asked to hold their forearms vertically and allow both hands to drop into complete flexion at the wrist for approximately one minute. In this position the median nerve is squeezed between the proximal edge of the transverse carpal ligament and the adjacent flexor tendons ad radius. Maintaining this position for a long time eventually causes numbness and tingling over the distribution of the median nerve
Phalen 1950
Vargas Busquets later recorded Phalen personally demonstrating the test in 1989, emphasising that the wrists should fall freely into flexion, with the hands not touching and not forced into position.
Modified Phalen test / dorsum-to-dorsum variant

The modified Phalen test places the dorsal surfaces of the hands together to maintain bilateral wrist flexion. A positive test reproduces or worsens numbness, tingling, pain, or paraesthesia in the median nerve distribution, usually within 60 seconds.
This dorsum-to-dorsum posture is a recognised variant, but was not Phalen’s original description. MacDermid and Wessel (2004) list the original gravity-assisted method and then describe variations including passive examiner flexion, wrist dorsums placed together to force both wrists into flexion, and combined manoeuvres with fist-making or carpal compression.
The transition from Phalen’s gravity-assisted wrist-flexion test to the now common dorsum-to-dorsum posture occurred gradually through clinical teaching and textbook illustration, rather than through a clearly attributed original publication. The modified posture probably became popular because it is easy to demonstrate, photograph, and visually standardise. However, this remains an inference rather than a documented reason.
Reverse Phalen test or Wormser test

The reverse Phalen test, or Wormser test, is a wrist-extension manoeuvre used in the evaluation of CTS. It is performed with the palms together in a “prayer” position, or with active wrist and finger extension. A positive test reproduces or worsens symptoms in the median nerve distribution.
In 1950, Peter Wormser discussed dorsiflexion of the wrist as a provocative or pathogenetic factor in Das Karpaltunnelsyndrom.
A reverse Phalen’s maneuver involves wrist and finger extension held for 1 minute. We showed that this maneuver results in a significantly higher intracarpal canal hydrostatic pressure as compared to a traditional Phalen’s or a modified Phalen’s maneuver.
In 1994, Robert A. Werner et al studied the Reverse Phalen’s maneuver as an aid in diagnosing carpal tunnel syndrome. Werner defined the it as wrist and finger extension held for one minute. They found that wrist/finger extension produced a higher intracarpal canal hydrostatic pressure than traditional Phalen or their own modified Phalen manoeuvre. They also reported symptom provocation in 55% of symptomatic CTS subjects and none of the controls.
Werner’s “modified Phalen” should not be confused with the modern dorsum-to-dorsum test. In their study, modified Phalen involved wrist flexion while pinching a flat object between the thumb and third digit.
Interpretation
A positive Phalen test supports, but does not prove, carpal tunnel syndrome. Symptoms should occur in the median nerve distribution of the thumb, index finger, middle finger, and radial half of the ring finger. Symptoms predominantly involving the little finger suggest ulnar nerve involvement or an alternative diagnosis.
A negative Phalen test does not exclude carpal tunnel syndrome. Phalen noted that the wrist-flexion test may be negative in advanced disease when sensory loss is already severe, and the test cannot be performed reliably when wrist flexion is restricted.
Diagnostic accuracy of Phalen test
Modern studies report variable accuracy, partly because “Phalen test” may refer to the original gravity-assisted wrist-flexion test, passive examiner flexion, dorsum-to-dorsum modified Phalen, or combined manoeuvres. Phalen’s own 1966 series reported the wrist-flexion test as positive in 380 of 515 hands tested (sensitivity 74%), but this was a clinical case series without a control group, so does not provide specificity.
Overall, the Phalen test is best regarded as a moderately useful provocative test for carpal tunnel syndrome, not a stand-alone diagnostic test. A positive result increases suspicion when symptoms are reproduced in the median nerve distribution; a negative result does not exclude carpal tunnel syndrome.
| Source | Test | Sensitivity | Specificity | Comment |
|---|---|---|---|---|
| Phalen 1966 | Classic wrist-flexion test | ~74% positive | N/A | Case series; 380/515 tested hands positive. |
| MacDermid 2004 | Phalen test systematic review | 68% | 73% | Noted variation in how Phalen’s test was performed. |
| Núñez de Arenas-Arroyo 2022 | Phalen test meta-analysis | 69% | 71% | Electrodiagnosis reference. Useful screening test, not definitive alone. |
| Dabbagh 2023 | Phalen test meta-analysis | 57% | 67% | Recommends combining with other clinical findings |
| Georgiew 2007 | Reverse Phalen | ~54% | ~78% | Lower sensitivity, higher specificity than classic Phalen |
| Goginava 2025 | Classic vs modified Phalen | Classic 93%; modified 96% | Classic 96%; modified 93% | Small direct comparison; broadly similar performance. |
Which version of Phalens test performs better?
Most diagnostic studies do not clearly separate the classic Phalen wrist-flexion test from later modified versions. The best direct comparison currently available is Goginava et al. 2025, which compared the classic gravity-assisted Phalen test with the modified dorsum-to-dorsum Phalen test in 21 women with idiopathic CTS and 21 controls, assessing 29 hands in each group. The classic Phalen was slightly more specific and the modified Phalen was slightly more sensitive. The study was small, so the safest conclusion is that both versions are clinically usable when performed consistently.
| Variant | Sensitivity | Specificity | Practical interpretation |
|---|---|---|---|
| Classic Phalen | 93% | 96% | Slightly higher specificity |
| Modified Phalen | 96% | 93% | Slightly higher sensitivity |
| Reverse Phalen / Wormser | ~54% | ~78% | Not superior, best used as an adjunct. |
The reverse Phalen test produced greater carpal tunnel pressure than wrist flexion in experimental pressure studies, but this has not translated into diagnostic superiority. Werner et al. showed that wrist and finger extension generated higher intracarpal canal pressure than traditional Phalen or their modified Phalen manoeuvre, yet symptom provocation occurred in only 55% of symptomatic CTS subjects.
Bottom line: use Phalen testing as part of a clinical examination for nocturnal paraesthesia, median-distribution symptoms, sensory change, thenar weakness or atrophy. Combine with Tinel sign, carpal compression testing, and electrodiagnostic studies for best accuracy. The exact Phalen test variant should be documented, because the “Phalen test” is not methodologically uniform across the literature.
History of the Phalen Test(s)
1948 – George Smith Phalen announced his diagnostic wrist-flexion test for carpal tunnel syndrome at a meeting of the American Society for Surgery of the Hand.
1950 – Peter Wormser published Das Karpaltunnelsyndrom. He discussed dorsiflexion of the wrist as a mechanical factor in median nerve compression and noted that strong passive dorsiflexion of the hand could sometimes elicit pain or dysaesthesia in the distal median nerve distribution (reverse Phalen test).
1951 – Phalen published Spontaneous compression of the median nerve at the wrist in JAMA.
1966 – Phalen published his 17-year Cleveland Clinic series, The carpal-tunnel syndrome, reviewing 654 hands in 439 patients. He illustrated the wrist-flexion test and reported it positive in 380 of 515 tested hands.
1970 – In Reflections on 21 years’ experience with the carpal-tunnel syndrome, Phalen reaffirmed the wrist-flexion test as one of the three major clinical signs of carpal tunnel syndrome, together with median-distribution hypoaesthesia and Tinel sign.
1994 – Miguel A. Vargas Busquets published a historical comment after meeting Phalen in 1989. He recorded and photographed Phalen’s own demonstration of the original test with elbows flexed, wrists falling freely into flexion, hands not touching, and no forced flexion.
1994 – Werner, Bir and Armstrong published Reverse Phalen’s maneuver as an aid in diagnosing carpal tunnel syndrome. They defined reverse Phalen as wrist and finger extension held for one minute and showed that it produced higher intracarpal canal pressure than traditional Phalen or their modified Phalen manoeuvre.
2004 – MacDermid and Wessel published a systematic review of clinical diagnosis in carpal tunnel syndrome listing multiple Phalen variants including the original gravity-assisted wrist-flexion test, passive examiner flexion, dorsum-to-dorsum wrist flexion, and reverse Phalen wrist extension.
2022–2023 – Modern meta-analyses confirmed that Phalen testing has moderate diagnostic accuracy and should be interpreted with history, sensory and motor examination, hand diagrams, questionnaires, and other provocative tests rather than used alone.
2025 – Goginava et al. directly compared classic and modified Phalen tests, finding similar diagnostic performance, with slightly higher sensitivity for modified Phalen and slightly higher specificity for classic Phalen.
Associated Persons
- George Smith Phalen (1911-1998)
Alternative names
- Phalen’s sign, Phalen’s test, Phalen’s maneuver
- Wrist-flexion test
- Reverse Phalen test
References
Historical articles
- Wormser P. Das Karpaltunnelsyndrom. Fortschritte der Neurologie, Psychiatrie und ihrer Grenzgebiete 1950; 18: 211-24.
- Phalen GS, Gardner WJ, Londe AA. Neuropathy of the median nerve due to compression beneath the transverse carpal ligament. J Bone Joint Surg Am. 1950; 32A(1): 109-12.
- Phalen GS. Spontaneous compression of the median nerve at the wrist. JAMA 1951;145:1128-1133.
- Phalen GS. The carpal-tunnel syndrome. Seventeen years’ experience in diagnosis and treatment of six hundred fifty-four hands. J Bone Joint Surg Am. 1966;48(2):211-228.
- Phalen GS. Reflections on 21 years’ experience with the carpal-tunnel syndrome. JAMA. 1970; 212(8): 1365-7.
Eponymous review
- Werner RA, Bir C, Armstrong TJ. Reverse Phalen’s maneuver as an aid in diagnosing carpal tunnel syndrome. Arch Phys Med Rehabil. 1994 Jul;75(7):783-6.
- Vargas Busquets MA. Historical commentary: the wrist flexion test (Phalen sign). J Hand Surg Am. 1994 May;19(3):521.
- Ghavanini MR, Haghighat M. Carpal tunnel syndrome: reappraisal of five clinical tests. Electromyogr Clin Neurophysiol. 1998 Oct-Nov;38(7):437-41
- MacDermid JC, Wessel J. Clinical diagnosis of carpal tunnel syndrome: a systematic review. J Hand Ther. 2004 Apr-Jun;17(2):309-19.
- Georgiew F. Provocative tests used in the diagnosis of carpal tunnel syndrome. Med Rehab. 2007;11(4):7-17.
- Bilkis S, Loveman DM, Eldridge JA, Ali SA, Kadir A, McConathy W. Modified Phalen’s test as an aid in diagnosing carpal tunnel syndrome. Arthritis Care Res (Hoboken). 2012 Feb;64(2):287-9.
- Núñez de Arenas-Arroyo S et al. Accuracy of the Most Common Provocation Tests for Diagnosing Carpal Tunnel Syndrome: A Systematic Review With Meta-analysis. J Orthop Sports Phys Ther. 2022 Aug;52(8):522-531
- Dabbagh A, MacDermid JC, Yong J, Packham TL, Grewal R, Boutsikari EC. Diagnostic Test Accuracy of Provocative Maneuvers for the Diagnosis of Carpal Tunnel Syndrome: A Systematic Review and Meta-Analysis. Phys Ther. 2023 Jun 5;103(6):pzad029.
- Goginava IB, Goloborod’ko SA, Riezunenko MV, Giorgidze GL. Phalen’s test. Classic or modern?. Ukrainian Neurosurgical Journal, 2025; 31(4): 68–73.
- Cadogan O. Clinical Signs in Carpal Tunnel Syndrome. LITFL
- Carpal Tunnel Exam. Stanford Medicine 25
eponymictionary
the names behind the name

Studying for Bachelor of Science (Occupational Therapy) at Curtin University
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |