
![]()
Risk and Numbers Needed to Treat
Revised and reviewed 26 August 2015
OVERVIEW
- Risk is a nebulous term in evidence-based medicine, as it may refer to either relative or absolute risks
- Overall, absolute risks are more meaningful and can be converted in ‘numbers need to treat’ (NNT), which are useful in the clinical setting
RISK
Absolute Risk
- the actual event rate in the placebo or treatment group
Relative Risk
- the ratio of the incidence of disease among exposed to the incidence among non-exposed
- a measure of the strength of an association between groups
- prospective studies (RCTs and cohort studies)
- also called the incidence risk
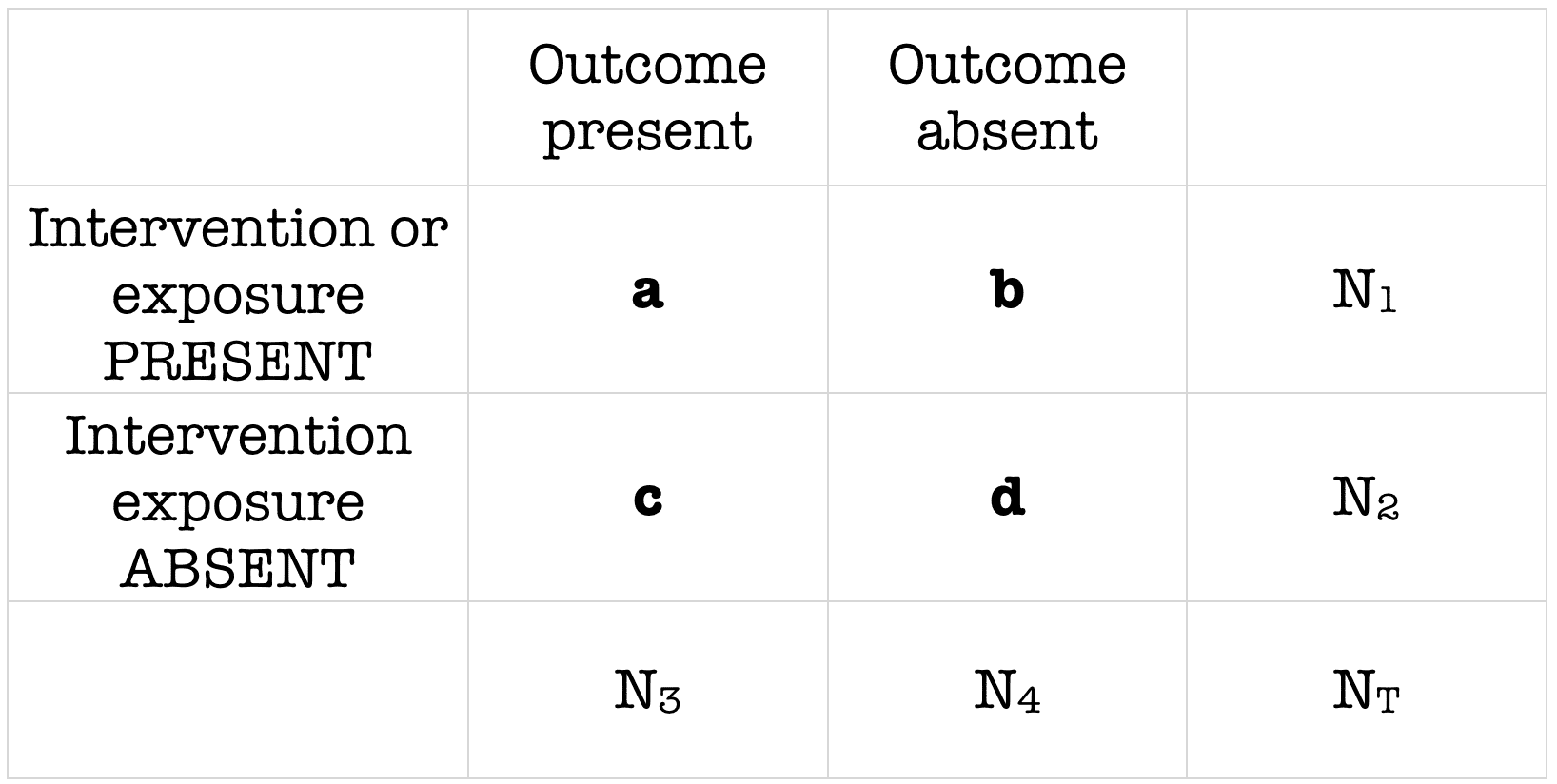
RR = risk of disease in the exposed (a/a+b) / risk of disease in the non-exposed (c/c+d)
- RR of 3 -> there is three times the risk
- RR of 0.5 -> the risk is halved
- RR of 1 -> there is no association
- if the RR is reported with a CI that includes 1 -> then the RR is not significant.
Relative Risk Reduction
- expressed as a percentage reduction in events in treated vs untreated groups
- = 1 – (incidence in exposed / incidence in unexposed)
Attributable Risk
- a measure of association that provides information about the absolute effect of the exposure or excess risk of disease of those exposed compared to unexposed
Absolute Risk Reduction (ARR)
- incidence in exposed – incidence in unexposed
- a measure of treatment effect
- reverse of attributable risk
NUMBER NEEDED TO TREAT
- NNT is the number of patients who need to be treated in order to avoid one adverse event, which is the reciprocal of the absolute risk reduction
- NNT gives the RR some relevance in terms of the magnitude of clinical effect
- ie. if the incidence of an adverse event = 0.06% & relative risk reduction = 0.33 the absolute risk reduction -> 0.02% and thus numbers needed to treat = 1/0.0002 = 5000
- however, if the incidence of an adverse event was 6% the absolute risk reduction -> 2% and thus the NNT = 1/0.02 = 50

Critical Care
Compendium
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
