![]()
Serotonin Syndrome
OVERVIEW
- Serotonin syndrome results from drug-induced over-stimulation of serotonin receptors in the CNS and is characterized by a triad of CNS dysfunction, autonomic disturbance and neuromuscular effects
- aka serotonin toxicity
CLINICAL FEATURES
- OD
- 2 or more serotonergic drugs (SSRI’s, TCA’s, MAO-I, St Johns Wort, methylene blue)
- onset usually within 24hrs
- venlafaxine is associated with the highest mortality rate among serotonergic agenics
Summary: altered mentation (CNS), autonomic dysfunction and neuromuscular hyperactivity (=CAN)
- CVS – tachycardia, hypotension/hypertension, flushing
- RESP – tachypnoea
- NEURO – confusion, seizures, coma, agitation, restlessness, clonus, hyperreflexia, incoordination, ataxia, rigidity, dilated pupils
- METABOLIC – fever
- HAEM – DIC
- RENAL – failure
HUNTER SEROTONIN SYNDROME CRITERIA
In the presence of a serotonergic agent:
- IF (spontaneous clonus = yes) THEN serotonin toxicity = YES
- ELSE IF (inducible clonus = yes) AND [(agitation = yes) OR (diaphoresis = yes)] THEN serotonin toxicity = YES
- ELSE IF (ocular clonus = yes) AND [(agitation = yes) or (diaphoresis = yes)] THEN serotonin toxicity = YES
- ELSE IF (tremor = yes) AND (hyperreflexia = yes) THEN serotonin toxicity = YES
- ELSE IF (hypertonia = yes) AND (temperature > 38ºC) AND [(ocular clonus = yes) or (inducible clonus = yes)] then serotonin toxicity = YES
- ELSE serotonin toxicity = NO
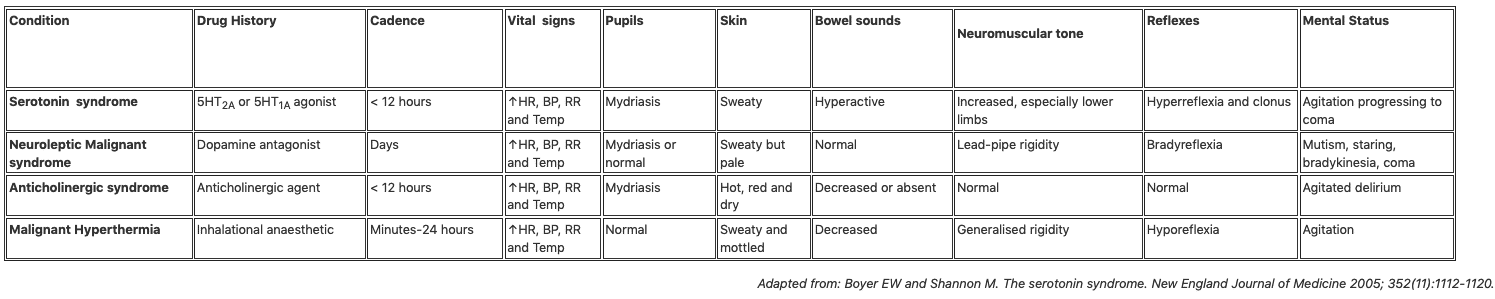
Important differences between serotonin syndrome and neuroleptic malignant syndrome:
1. NMS is a idiosyncratic reaction after prolonged exposure to neuroleptics or after withdrawal of a dopamine receptor agonist.
2. NMS usually develops over days or weeks
3. NMS usually accompanied by hyperthermia, severe muscle rigidity and rhabdomyolysis (not mydriasis, diarrhoea, hyperreflexia, myoclonus)
4. NMS frequently associated with multi-organ failure
MANAGEMENT
Resuscitate
- seizure or coma -> intubation
- terminate seizures with benzodiazepine
Specific Treatment
- indicated if marked hyperthermia, rhabdomyolysis, DIC, renal failure, ARDS -> cyproheptadine and chlorpromazine
- cyprohepatidine – antihistamine with antiserotonergic action.
- olanzepine
Underlying cause
- single dose of charcoal if presents within 1 hr
- discontinue all serotonergic medications
- usually subsides over 24 hrs but deaths have been reported
Differential
References and Links
CCC Toxicology Series
General
Approach to acute poisoning, ECGs in Tox, Evidenced-based Tox, Toxicology literature summaries, Does anti-venom work?
Toxins / Overdose
Amphetamines, Barbituates, Benzylpiperazine, Beta Blockers, Calcium Channel Blocker, Carbamazepine, Carbon Monoxide, Ciguatera, Citrate, Clenbuterol, Cocaine, Corrosive ingestion, Cyanide, Digoxin, Ethanol, Ethylene Glycol, Iron, Isoniazid, Lithium, Local anaesthetic, Methanol, Monoamine oxidase inhibitor (MAOI), Mushrooms (non-hallucinogenic), Opioids, Organophosphate, Paracetamol, Paraquat, Plants, Polonium, Salicylate, Scombroid, Sodium channel blockers, Sodium valproate, Theophylline, Toxic alcohols, Tricyclic antidepressants (TCA)
Envenomation
Marine, Snakebite, Spider, Tick paralysis
Syndromes
Alcohol withdrawal, Anticholinergic syndrome, Cholinergic syndrome, Drug withdrawals in ICU, Hyperthermia associated toxidromes, Malignant hyperthermia (MH), Neuroleptic malignant syndrome (NMS), Opioid withdrawal, Propofol Infusion Syndrome (PrIS) Sedative toxidrome, Serotonin syndrome, Sympatholytic toxidrome, Sympathomimetic toxidrome
Decontamination
Activated Charcoal, Gastric lavage, GI Decontamination
Enhanced Elimination
Enhanced elimination, Hyperbaric therapy for CO
Antidotes
Antidote summary, Digibind, Glucagon, Flumazenil, HIET – High dose euglycaemic therapy, Intralipid, Methylene Blue, N-Acetylcysteine (NAC), Naloxone
Miscellaneous
Cocaine chest pain, Digoxin and stone heart theory, Hyperbaric oxygen, Hypoxaemia in tox, Liver failure in tox, Liver transplant for paracetamol, Methaemoglobinaemia, Urine drug screen
- Sternbach H. The serotonin syndrome. Am J Psychiatry. 1991 Jun;148(6):705-13.
- Dunkley EJ, Isbister GK, Sibbritt D, Dawson AH, Whyte IM. The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity. QJM. 2003 Sep;96(9):635-42
- Boyer EW, Shannon M. The serotonin syndrome. The New England journal of medicine, 2005;352 (11), 1112-20
- Isbister GK, Buckley NA, Whyte IM. Serotonin toxicity: a practical approach to diagnosis and treatment. Med J Aust. 2007 Sep 17;187(6):361-5.
- Torre LE, Menon R, Power BM. Prolonged serotonin toxicity with proserotonergic drugs in the intensive care unit. Crit Care Resusc. 2009 Dec;11(4):272-5

Critical Care
Compendium
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC