
![]()
Something’s not right…
aka Cardiovascular Curveball 004
A 26 year-old man presented to the ED with chest pain, He tripped on some steps and the right-side of his chest collided with the handrail.This is his chest radiograph:
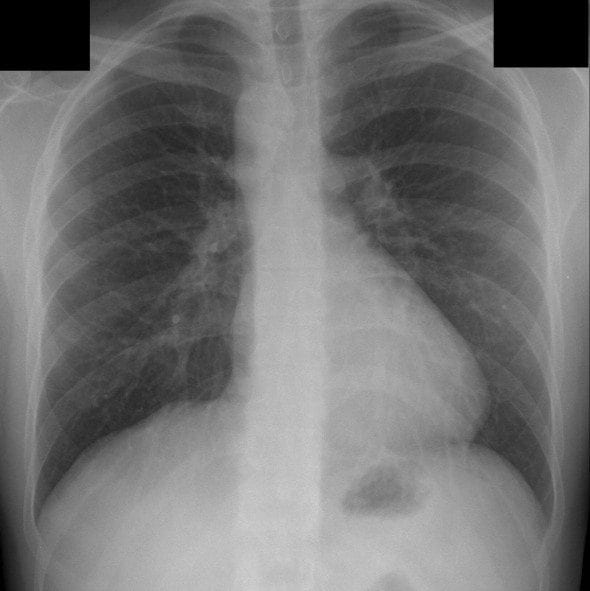
Q1. What are the chest radiograph findings?
Curveball Answer
There is a right-sided aortic arch.
- The trachea is deviated to the left of the midline rather than the right.
- There is no evidence of traumatic injury or situs inversus.
- About 1 in 100,000 people have a right-sided aorta. It occurs during embryological development when the left 4th branchial arch involutes and the right remains, rather than vice versa.
- Right-sided aortic arch can simply be mirror image of a normal left-sided arch, in which case situs inversus may also be present. Alternatively, the right-sided arch may give rise to a left subclavian artery that passes leftwards behind the esophagus, or the arch may cross over into a normal left-sided descending thoracic aorta.

Q2. What is the significance of this radiographic finding?
Curveball Answer
Right sided aortic arches are asymptomatic if they occur in the absence of other cardiovascular abnormalities.
However, if a right-sided aortic arch is present, other abnormalities such as Tetralogy of Fallot (20% have a right-sided aortic arch) and truncus arteriosus may also be present.
These abnormalities are more likely with right-sided aorta arches of the ‘mirror image’ type.
Q3. If a child has this finding and presents with respiratory distress or dysphagia what should be suspected?
Curveball Answer
Obstruction from a vascular ring encircling and constricting the trachea and /or oesophagus.
- For instance, a ring forms around the trachea and oesophagus when a left-sided ligamentum arteriosum connects the left pulmonary artery and a retroesophageal left subclavian artery arsing from the right-sided aortic arch.
- This can mimic croup or recurrent respiratory tract infections – the diagnosis requires a high index of suspicion.
- Bronchoscopy and barium esophagraphy help define the extent of airway or oesophageal compression.
- Echocardiography and/or cardiac catheterisation may also be used to define the nature of any cardiovascular anomalies associated with the vascular ring. CT or MRI may also be performed.
- The ring can be released by division of the ligamentum arteriosum.
Q4. What is the diverticulum of Kommerell?
Curveball Answer
The diverticulum of Kommerell is a dilated pouch at the aortic origin of the retroesophageal left subclavian artery.
- It is formed from the remnant of the involuted left branchial arch.
- Its presence makes the vascular ring tighter, increasing compression of the trachea and oesophagus.
- Thus, right-sided aortic arches that have vascular rings associated with a diverticulum of Kommerell are more likely to be symptomatic.
References
- Yamamoto LG. Radiology Cases in Pediatric Emergency Medicine
- Grainger and Allison’s Diagnostic Radiology
- Nadas’ Pediatric Cardiology
- Yamamoto LG. Difficulty Breathing Throughout Infancy. Radiology Cases in Pediatric Emergency Medicine Volume 6, Case 19

CLINICAL CASES
Cardiovascular Curveball
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC