
![]()
Taipan
Taipan envenomation is usually lethal without antivenom treatment. It classically causes a rapid venom induced consumptive coagulopathy (VICC), neurotoxicity and myotoxicity.
The different taipans include: Inland taipan, small-scaled or fierce snake, Papuan taipan, costal taipan and central ranges taipan.
Resus
Potential life threats include (the patient should initially be managed in an area capable of resuscitation):
- Cardiac arrest – undiluted antivenom should be given as a rapid push 1 ampoule and continue with advanced life support along usual guidelines
- Hypotension
- Rapid onset paralysis with respiratory failure
- VICC with uncontrolled haemorrhage
- Seizures
Risk Assessment
Typical symptoms include:
- Minimal signs of a bite or the patient maybe unaware they have been bitten
- Systemic features include headache, nausea and vomiting.
- The first sign of envenomation maybe collapse
- Paralysis is usually evident within 1-2 hours (descending, symmetrical, look for ptosis, blurred vision, diplopia and difficulty swallowing)
- Clinical signs of a VICC include bleeding gums, haemorrhage at the IV sites or intracranial/intra abdominal
- Myotoxicity will present as myalgias, myoglobinuria and progressive renal failure
- Thrombotic microangiopathy (TMA): Thrombocytopenia, microangiopathic haemolytic anaemia (MAHA) and acute renal failure
- Patients do not require the complete triad of paralysis, coagulopathy and myotoxicity to confirm Taipan envenomation
Supportive Care
1. IV fluids – for myotoxicity and to help prevent complications from myoglobinuria
2. Intubation and ventilation – if paralysis is causing respiratory failure.
3. Pressure bandage with Immobilisation (PBI) – Should have been applied pre-hospital, if not apply while awaiting initial investigations.
PBI Video
Investigations
1. Laboratory Tests (At presentation, 1 hour post PBI removal, 6 and 12 hours following the bite): FBC, EUC, CK, INR, APTT, Fibrinogen, D-dimer. If there is no evidence of envenoming at 12 hours after the bite, the patient is fit for discharge (although not during the night as subtle neurotoxicity maybe missed).
2.Taipans cause a Complete or partial VICC which usually resolves after 10 -20 hours (INR <2)
- Elevated INR >3 (or max or undetectable)
- Undetectable fibrinogen
- Elevated INR (max or >10 x normal)
3.Partial VICC:
- Elevated INR but
- Low but detectable fibrinogen
4. Monitor renal function and evidence of myotoxicity (CK and myoglobinuria) and MAHA (raised LDH and fragmented red blood cells – only need to do if the patient has been envenomed)
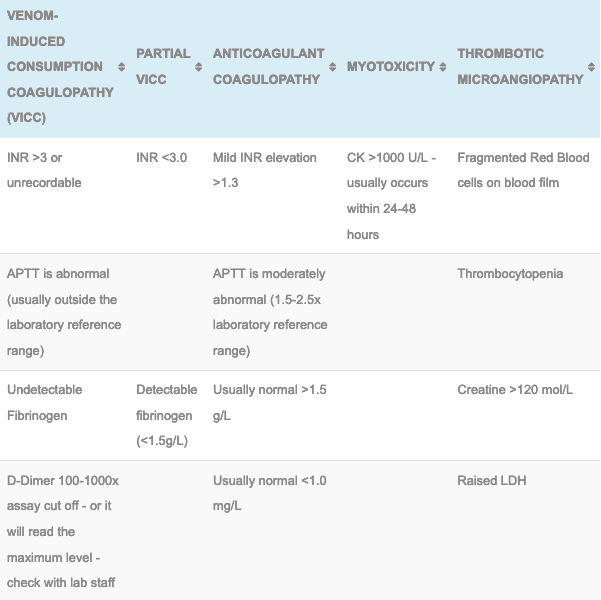
Laboratory Results seen in the Australian Snake Envenomations
5. The Snake Venom Detection Kit (SVDK): This is not used to diagnose envenoming but can be used to determine which monovalent antivenom to use if more than one snake could be responsible for the observed clinical features. This kit does produce false positives and false negatives, caution needs to be used and contacting a clinical toxicologist is highly recommended if your patient is envenomed.
Differential Diagnosis:
- Brown sales are in the same geographical area and can cause a VICC but paralysis and myotoxicity is rare
- Tiger snakes and Taipans can co-exist in parts of Queensland with similar presentations, usually the myotoxicity and paralysis takes hours to manifest
- Death Adders can cause a descending flaccid paralysis but myotoxicity and coagulation defects do not occur.
Antivenom
- 1 amp of CSL monovalent Taipan Snake Antivenom: Used in the treatment of envenomation (systemic symptoms, laboratory evidence of complete or partial VICC or paralysis) by taipan snake
- See Taipan antivenom for dosing, administration and complication details
Disposition
- All patients must be observed in a hospital capable of managing a potential snake bite envenomation, this involves adequate laboratory cover and the ability to administer antivenom and manage potential anaphylaxis.
- Patient with no laboratory evidence of VICC and no clinical evidence of neurotoxicity at 12 hours post bite are not envenomed and maybe discharged in daylight hours.
- Envenomed patients can be discharged following antivenom and resolving coagulation (INR <2), mild and stable neurological findings and a falling CK with no evidence of renal failure or MAHA
Controversies
- Administration of antivenom does not appear to hasten the recovery from VICC, but it may reverse or prevent other manifestations of envenoming.
- Plasmapheresis has been used to treat thrombotic microangiopathy but its utility is still undefined.
- Administration of Fresh Frozen plasma or cryoprecipitate after antivenom administration is associated with earlier recovery from VICC but it does not effect time to discharge and the exact utility to this approach has not be well defined in clinical practice.
References and Additional Resources:
Additional Resources:
- Taipan Antivenom
- Approach to the Snakebite Patient
- Tox Conundrum 005 – Snakebite vs Stickbite
- Tox Conundrum 026 – Snakebite Envenoming Challenge
Zeff – James Hayes Fellowship teaching Snakebite
References:
- Isbister GK, Buckley NA, Page CB et al. A randomised controlled trial of fresh frozen plasma for treating venom-induced consumption coagulopathy in cases of Australian snakebite (ASP-18). Journal of Thrombosis and Haemostats 2013; 11:1310-1318
- Sutherland SK, Timbals J. Australian animal toxins: the creatures, their toxins and care of the poisoned patient. South Melbourne: Oxford University Press; 2001
- Trevett AJ, Lalloo DG, Nwokolo NC et al. The efficacy of antivenom in the treatment of bites by the Papuan Taipan (Oxyuranus scutellatus canni). Transactions of the Royal Society of Tropical Medicine and Hygiene 1995; 89:322-325
- White J. A clinician’s guide to Australian venomous bites and stings: Incorporating the updated CSL antivenom handbook. Melbourne: CSL Ltd, 2012

Toxicology Library
TOXINS
Dr Neil Long BMBS FACEM FRCEM FRCPC. Emergency Physician at Kelowna hospital, British Columbia. Loves the misery of alpine climbing and working in austere environments (namely tertiary trauma centres). Supporter of FOAMed, lifelong education and trying to find that elusive peak performance.
